Actinomyces - Lab diagnosis, Prevention, Control, Treatment
Laboratory diagnosis of Actinomyces
The laboratory diagnosis of Actinomyces includes:
Specimen/Samples
Specimens for the detection of actinomycosis due to Actinomyces include
sputum
bronchial secretion
discharge
infected tissue (which may contain large no. of sulfur granules)
* Transportation must be done immediately under anaerobic conditions.
Microscopy
Material from suspected cases is shaken with sterile water in a tube. Sulfur granules of Actinomyces settle to the bottom which is removed. Granules are then crushed between two sides and stained by Gram and Z-N stain (with 1% H2SO4 for decolorization) method.
Gram-positive hyphal fragments surrounded by a peripheral zone of swollen, radiating, club-shaped structures presenting a sunray appearance are revealed in infected specimens.
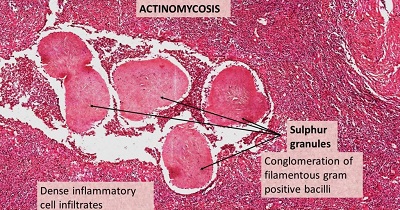
Fig: Actinomyces sulphur granules (Source: ilovepathology)
Culture
A culture of pus or sulfur granules of Actinomyces is done in BHI + 5% serum, thioglycolate broth, and blood agar. The incubation is done at 35-37°C, with 10% CO2 for 7-14 days.
The Actinomyces israeli colony is around 5mm in diameter, shite smooth, entire, or lobulated colonies resembling molar teeth or lobulated colonies resembling molar teeth after 10 days of incubation.
Molecular
Molecular methods for Actinomyces include:
DNA probes
PCR
Histological examination
The sample is a lung biopsy. The gold standard is the presence and detection of sulfur granules.
CT-scan
Chest CT scans may be confused with malignancy (mars) or tuberculosis. It consolidates actinomycosis, caused by Actinomyces spp., detection but not the procedure for confirmation.
Identification
Microscopy
Suger utilization test
Direct fluorescent microscopy
Gel diffusion test (Ouchterlony)
Prevention, Control, Treatment of Actinomyces
Good dental and oral hygiene
High dose penicillin (peri G) or tetracycline for a long time
Cephalosporins or Amoxycillin
IV 18-24 million units/day of PenG for 2-6 weeks followed by oral therapy with PenV or amoxicillin for 6-12 months.