Mycobacterium tuberculosis - Clinical manifestation, GHON’s COMPLEX, Primary, Secondary, Extrapulmonary tuberculosis
Clinical manifestation of Mycobacterium tuberculosis
Clinical manifestation in patients infected with Mycobacterium tuberculosis complex may range from symptomatic to acutely symptomatic. Symptomatic patients can have systemic symptoms, pulmonary signs, and symptoms, signs, and symptoms related to other involved organs, or a combination of them.
The clinical syndromes of tuberculosis include:
Primary tuberculosis
Secondary (post-primary) tuberculosis
Extrapulmonary tuberculosis/chronic pulmonary tuberculosis
Primary tuberculosis
The infection of an individual who has not been previously infected falls under primary tuberculosis.
The common symptoms include low-grade fever, night sweats, fatigue anorexia, weight loss, cheesy sputum production with tingled blood, chills, myalgia (muscle pain), sweating, and hemoptysis (blood in cough).
It is the initial infection by the tubercle bacilli in the lungs after 3-8 weeks from the time of infection. The lower lobe or lower part of the upper lobe is involved. A necrotic lesion is formed at the site of infection called Ghon’s focus.
In the majority of cases, the lesion heals spontaneously leaving behind a calcified nodule. Inside the healed lesion, few bacilli may survive and remain latent which might cause disseminated tuberculosis called extrapulmonary tuberculosis.
GHON’s COMPLEX (Primary complex)
Consists of three components
Pulmonary component (Ghon’s focus)
Lymphatic components
Lymph node component – Hilar and Tracheobronchial
Pulmonary component
The pulmonary component (Ghon’s focus) or primary focus is a lesion in the lung. The lesion, which is about 1-2 cm solitary area, is located peripherally in the subpleural focus in the lower part of the lower lobe or upper part of the lower lobe.
Lung lesions show tuberculous granola with caseous necrosis.
Lymphatic component
Lymphatic components are caused by lymphatics draining lung lesions containing phagocytes with Mycobacterium tuberculosis bacilli.
Lymph node component
Lymph node components are enlarged hilar and tracheobronchial lymph nodes. The affected lymph nodes may show caseation necrosis which can be a potential source of reinfection later.
* The fate of primary tuberculosis:
Heal by fibrosis => calcification
Progressive primary tuberculosis
Primary miliary tuberculosis
Secondary (post-primary) tuberculosis
Secondary (post-primary) tuberculosis occurs due to the reactivation of latent infection or exogenous reinfection. Mainly upper lobes of the lungs are involved and symptoms include- fatigue, anorexia, night fever, hemoptysis, and unwanted weight loss.
Dissemination of the bacterium may occur via the lymph system or hematogenous leading to meningeal or miliary (disseminated) tuberculosis. This occurs in patients with depressed or ineffective cellular immunity.
The following organs may be involved:
Genitourinary tract
lymph nodes (cervical lymphadenitis)
CNS (meningitis)
Bone and joints (arthritis and osteomyelitis)
peritoneum
pericardium
larynx
pleural lining (pleuritis)
HIV patients are susceptible to developing active tuberculosis. They are likely to have rapidly progressive primary disease instead of subclinical infection. Chest infection of HIV patients for pulmonary disease lack specificity and patients are frequently anergic (lack biological response) to tuberculin skin testing.
Secondary tuberculosis, caused by Mycobacterium tuberculosis, differs from primary tuberculosis in the following features:
granulomas of secondary tuberculosis occur more commonly in the upper lobes of the lungs
involvement of the lymph nodes as usual
the cavities may rupture into blood vessels, causing dissemination of mycobacteria in the body or these may rupture into airways, releasing mycobacterium in aerosol and sputum
* The fate of secondary tuberculosis
The lesion may heal with fibrous scarring and calcification
Fibrocaseous tuberculosis (progressive pulmonary TB)
Tuberculous caseous pneumonia
Miliary tuberculosis
Fibrocaseous tuberculosis:
Fibrocaseous tuberculosis, caused by Mycobacterium tuberculosis, is seen usually in elderly, immunosuppressed people, or untreated patients. Apical lesion enlarges with the expansion of the area of necrosis forming a cavity that may either.
break into the bronchus from a cavity with the evacuation of caseous material (open fibrocaseous TB)
break into blood vessels producing hemoptysis
the cavity provides a favorable environment for the proliferation of bacilli due to high oxygen tension
the open case of secondary TB may implant tuberculosis lesions on the mucosal lining of air passages producing endobronchial/endotracheal TB.
Lung TB- cavitation
Miliary pulmonary tuberculosis
Miliary pulmonary tuberculosis occurs when organisms drain through lymphatics into lymphatic ducts to venous return on the right side of the heart and finally to pulmonary arteries.
Individual lesions are either microscopic or visible (2mm) foci of yellow-white consolidation scattered through the lung parenchyma (resembling millet seeds). The lesion, caused by Mycobacterium tuberculosis, shows the structure of a granuloma with minute areas of caseous necrosis.
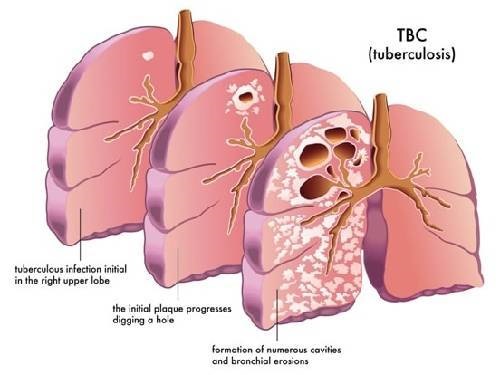
Fig: Tuberculosis in humans (Source: Practo)
Extrapulmonary tuberculosis/chronic pulmonary tuberculosis
Extrapulmonary tuberculosis/chronic pulmonary tuberculosis occurs in 10% of patients and may occur years after primary infection.
The accumulation of a large concentration of mycobacterial antigen leads to extensive and continuous CD4 + Tcell activation ensuing in macrophage activation. The resulting high concentration of lytic enzymes causes necrotic caseous lesions to liquefy. The liquefied substance provides a rich medium allowing the tubercle bacilli to multiply extracellularly.
The lesions rupture and the Mycobacterium tuberculosis bacilli disseminate in the lungs or spread through blood and lymphatic vessels to the bone, joints, urogenital system, meninges, etc. The following organs may be involved:
Genitourinary tract
lymph nodes (cervical lymphadenitis)
CNS (meningitis)
Bone and joints (arthritis and osteomyelitis)
peritoneum
pericardium
larynx
pleural lining (pleuritis)
Depending upon the site of Mycobacterium tuberculosis infection, extrapulmonary tuberculosis may be:
Genitourinary tuberculosis
Tubercular meningitis
Gastrointestinal tuberculosis
Skeletal tuberculosis
Tubercular lymphadenitis
Other conditions
Genitourinary tuberculosis
Genitourinary tuberculosis, caused by Mycobacterium tuberculosis, is one of the most common extrapulmonary manifestations of tuberculosis. The typical symptoms include dysuria, increased frequency of urination, and flank pain (discomfort in the upper abdomen, back, and sides).
The condition in men may manifest as epididymitis or a growth in the scrotal area. In women, the condition may manifest as PID. Genitourinary tuberculosis is responsible for approximately 10% of the sterility of women.
Tubercular meningitis
Tubercular meningitis is one of the most severe complications of tuberculosis. This condition may manifest as a headache, which is either intermittent or persistent.
Gastrointestinal tuberculosis
The clinical manifestation, of gastrointestinal tuberculosis, of the condition depends on the site affected in the GI tract. For example, infection of the stomach or duodenum manifests as abdominal pain mimicking peptic ulcer disease. Whereas Mycobacterium tuberculosis infection of the large intestine manifests as pain in the abdomen, diarrhea, etc.
Skeletal tuberculosis
In skeletal tuberculosis, the spine is the most common site resulting in pott’s disease
Tubercular lymphadenitis:
Tuberculous lymphadenitis (or tuberculous adenitis) is a chronic specific granulomatous inflammation of lymph nodes with caseation necrosis, caused by infection with Mycobacterium tuberculosis or Mycobacterium bovis.
It most commonly involves the neck along with the sternocleidomastoid muscle.
Other conditions
These include miliary tuberculosis (widespread via blood), tuberculosis of the skin, tuberculosis of the middle ear, and ocular tuberculosis.