Mycobacterium tuberculosis - Lab diagnosis, Sputum, Microscopy, Grading, Culture, PPD test
Laboratory diagnosis of Mycobacterium tuberculosis
The laboratory diagnosis of Mycobacterium tuberculosis begins with the collection of samples or by imaging.
Sample
Sputum (collected early morning for 3 regular days)
BAL
bronchial/tracheal aspirates (in the case of extrapulmonary tuberculosis)
urine
gastric aspirates
biopsy specimen
CSF
pericardial and pleural fluid bone marrow
blood feces from immunocompromised patients
Things to remember
the gastric aspirate was collected in cases of difficulty in sputum production (in case of child patients)
stimulation of cough can be done by using an aerosol solution of propylene glycol in 10% sodium chloride
CSF is collected for diagnosis of tubercular meningitis
Urine is for genitourinary tuberculosis. Urine specimens are centrifuged at 300 rpm for 30 mins and sediments are used for culture and microscopy
*Acid-fast bacilli can infect almost any tissue organ
Collection of sputum
When sputum is collected, the following procedure must be followed
The patient is provided with a clean, dry, wide-necked, leak-proof container and requested to produce a sputum specimen
If the patient is young or in cases in which sputum was swallowed during the night, gastric lavage can be collected
The container must be labeled and the request form must be filled out before being dispatched to the processing
Processing of sputum
After collection, the sputum must be processed as
A smear (of sputum sample) is prepared on a slide for Ziehl-Neelson’s staining using any caseous particles and the most purulent materials. The slide is then allowed to dry in a safe place
The slide is fixed by using 1-2 drops of 70% ethanol
The slide is covered with filtered carbon fuschin stain
The stain is heated until the vapor just begins to rise
Allow the heated stain to remain on the slide for 5 mins
Wash well with clean water
Cover the smear with 3% v/v acid alcohol for 5 mins and wash well with clean water
Cover the smear with malachite green for 1-2 mins then wash with clean water
Blot dry the back of the slide and place it in the rack
Observe under oil immersion at 100x (pleural fluid, peritoneal fluid, and other exudates are collected in containers with citrate to prevent coagulation.)
* specimens should be transported asap. In case of delay, specimens are refrigerated at 4°C but not more than overnight.
Transport medium: 1% cetyl Dyridenium Chloride (CPC) + 2% NaCl or Tri Sodium Phosphate
Microscopy
microscopy is a sensitive and rapid procedure for the presumptive identification of Mycobacterium tuberculosis
presumptive identification
the cell wall of mycobacteria contains long-chain, multiply cross-linked fatty acids, called mycolic acids
The mycolic acids and lipids in the mycobacterial cell wall account for its resistance to drying and harsh decontamination agents
low sensitivity stains both alive and dead mycobacterium (requires 104- 105) bacilli per ml of sputum
3 types of staining procedures can be used:
Fluorochrome stain (most sensitive)
Ziehl-Neelsen stain / carbolfuchsin stain
Kinyoun stain (cold stain procedure)
In Z-N stain, Mycobacterium spp. Appear red or red-blue, beaded appearance whereas non-mycobacteria appear blue
A procedure similar to Z-N stain but no heat is used. Acid-fast bacilli appear purple to read, slightly curved, short or long rods (2-8 μm). They also may appear beaded or banded.
cross-contamination of slides during the staining process and the use of water contaminated with saprophytic mycobacteria can lead to false-positive results.
Grading of ZN-stained smears for AFB
Field | No. of microorganisms | Interpretation |
|---|---|---|
1 field | More than 10 | 3+ |
1 field | 1-10 | 3+ |
100 field | 10-100 | 1+ |
100 field | 1-9 | Report exact number |
300 field | 0 | AFB not seen |
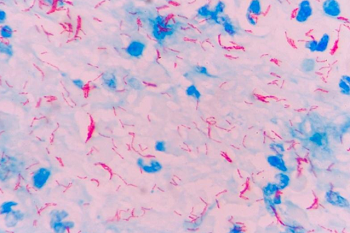
Fig: Mycobacterium tuberculosis ZN staining (Source: Semantic Scholar)
Culture
The culture of Mycobacterium tuberculosis can be done by:
Media used:-
Lowenstein-Jensen (LJ medium) = egg-potato based (solid media)
Middlebrook 7H10 medium = serum / albumin-based (solid media)
Mycobacteria Growth Indicator tube (MGIT) (liquid media)
One solid medium and one liquid medium is considered a standard culture procedure but is usually impractical
More sensitive than microscopy
The advantage of liquid media is that bacilli grow in approximately 10 days, compared with 17 days or longer incubation time
10-100 AFB per ml of culture rather than Petri plate so as to reduce exposure of tubercle bacilli with air thus limiting lab-acquired infection
Process:
The procedure for culture of Mycobacterium tuberculosis are as follows:
About 20 min before culturing, the specimen is decontaminated by mixing the specimen (sputum) with the volume of NaOH (40g/l). It is mixed at intervals to homogenize the sputum
Using a sterile Pasteur pipette, 200 μl of well-mixed sputum sample is inoculated on a slope of LJ medium and the specimen is allowed to run down the slope.
The inoculated medium is incubated at 35-37°C in 5-10% CO2 atmospheric and high humidity in a rack placed at an angle of 45°C to ensure the full length of the slope is covered.
After 1 week the slope is placed in an upright position and further incubated for 5-10 weeks examining twice a week for growth.
Cultures should not be discarded as negative until they have been observed for 12 weeks
The screw cap of the LJ medium can be left loose for the first week of incubation to allow the evaporation of excess fluid and entry of CO2.
Mycobacterium tuberculosis is indicated by rough, buff, and tough colonies

Source: Mycobacterium tuberculosis on Löwenstein-Jensen medium (Source: Bacteria in Photos)
Antigen-protein detection
Detection of microbial products/components has been used to diagnose infection caused by Mycobacterium tuberculosis.
Eg: Tuberculostearic acid (a fatty acid that can be extracted from the mycobacterial cell wall) is detected by gas chromatography or mass spectrometry in specimens containing few mycobacteria
It can also be used in cases of tuberculous meningitis (CSF sample).
A host enzyme Adenosine deaminase is increasingly produced in patients with tuberculous pleural effusions. This enzyme detection is a form of diagnosis (sensitive= 98%, specificity = 96%)
Immunodiagnostic testing
Interferon-gamma release assays (eg: T-SPOT-TB, QuantiFERON – TB gold) are being used for the diagnosis of tuberculosis.
For immunodiagnostic testing, Mycobacterial Ag such as BCG, 5 and 6 kDa protein of Mycobacterium tuberculosis, 34 and 64 kDa protein of M. bovis is used
Advantages
Do not cross-react with non-tuberculous mycobacterium
are not affected by the BCG vaccine
are not variable as the serologic tuberculin skin test
* T-SPOT-TB does not require a follow-up visit with a physician and it measures T-cells that have been activated by Mycobacterium tuberculosis Ag.
* Quanti-FERON gold (a type of ELISA) measures a component of CMI (cell-mediated immunity) response to M. tuberculosis to diagnose latent and active tuberculosis
Tuberculin skin test / purified protein derivative (PPD) test
After infection by Mycobacterium tuberculosis, the individual develops a delayed hypersensitivity to certain Ag of the microorganism that can be detected by the Tuberculin skin test / purified protein derivative (PPD) test.
Procedure:
The procedure for Tuberculin skin test / purified protein derivative (PPD) test includes:
0.1 ml culture extract of Mycobacterium tuberculosis i.e. PPD of tuberculin containing 5 TU (tuberculin units) is injected intracutaneously in one arm
Option: 0.1ml of sterile normal saline is injected intracutaneously into another arm as a control
Delayed type hypersensitivity reaction to PPD is observed after 48-72 hours and characterized by erythema (redness) and firmness
Its firmness (induration) is measured and interpreted as:
10 mm or above = positive
5 mm or less = negative
6-9 mm = equivocal
Interpretation criteria are different in different patient populations (eg: immunosuppressed individuals – with AIDS)
DTH (delayed-type hypersensitivity) is observed in patients who have had the BCG vaccine
PPD test is not 100% specific or sensitive
False-negative test (anergy) can be seen in conditions such as miliary tuberculosis, convalescence form of some viral infection like measles, lymphoreticular malignancy, severe malnutrition, impaired CMI, immunosuppressive therapy
*(If the test is negative using 5 TU, can be repeated using 10 TU or 100 TU)
Pigment production
If the culture of Mycobacterium tuberculosis is left in light (not direct sunlight) for 2 hours and then reincubated at 35-37°C, it produces yellow pigment.
Molecular methods
Commonly used molecular methods for Mycobacterium tuberculosis diagnosis are:
PCR
Restriction fragment length polymorphism (RFLP)
DNA microarrays
TCH test
TCH (Thiophene-2-carboxylic acid hydrazide) inhibits the growth of some mycobacteria
This test is used to distinguish Mycobacterium tuberculosis (is not inhibited by TCH) from M. bovis (inhibited by TCH)
Other tests
Neutral red test: positive
Catalase test: Positive (weekly)
Aryl sulfate test = Negative
Nitrate reduction = strongly positive
Amidase test = Positive
Niacin test = Positive