Mycoplasma hominis - Introduction, Classification, Morphology, Clinical Syndrome
Classification of Mycoplasma hominis
Classification of Mycoplasma hominis can be done phenotypically.
Domain: Bacteria
Phylum: Mycoplasmatota
Class: Mollicutes
Order: Mycoplasmatales
Family: Mycoplasmataceae
Genus: Mycoplasma
Species: hominis
Introduction to Mycoplasma hominis
Mycoplasma hominis is a facultative anaerobe that is fast-growing (within 1-4 days) and is able to metabolize arginine but does not utilize glucose. It produces a large fried egg appearance colony on Mycoplasma media.
It inhabits the mucosa of the urogenital tract. To differentiate it from other genital Mycoplasma spp., inhibition of the growth of the bacteria with specific antisera is done.
Morphology of Mycoplasma hominis
The common morphological features of Mycoplasma hominis include:
gram-negative (very poorly stained)
size 0.3x0.8 micrometer (passes through 0.45micrometer filter)
lack cell wall
the cell membrane is 3 layered and contains sterols (eg. Cholesterol) which are supported by cytoskeleton and protein networks
two forms – filamentous and granular
lacks flagella or pilli but exhibits gliding motility
multiplication by binary fission
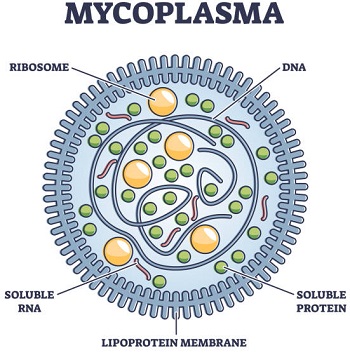
Fig: Mycoplasma hominis morphology (Source: iStock)
Clinical syndrome of Mycoplasma hominis
Clinical manifestations of Mycoplasma hominis, also known as Genital mycoplasma, vary depending on the type of infection.
It causes urogenital infections resulting in manifestations such as salpingitis (infection of the fallopian tube), pelvic abscess, puerperal (postpartum) infection, septic abortion, prostatitis, PID, amnionitis, non-gonococcal urethritis, acute pyelonephritis.
It may also cause primary atypical pneumonia, meningitis in newborns, arthritis, peritonitis, thrombophlebitis, and brain abscess.
Incidence of colonization by genital mycoplasmas increases after puberty as a result of sexual contact
In neonates, transmission occurs from colonized mother by ascending route to the newborn infant (urogenital tract), by crossing the placenta by delivering through a colonized birth canal, or postnatally from mother to infant. Meningitis, abscess, bacteremia, and pneumonia can be observed
In immunosuppressed patients, it takes an invasive form. Bacteremia, arthritis, pneumonia, peritonitis, abscesses, and other wound infections.