Bacterial vaginosis - Introduction, Clinical Syndromes, Lab Diagnosis
Introduction to bacterial vaginosis
Bacterial vaginosis is an unpleasant but mild condition characterized by malodorous (unpleasant smell) vaginal discharge due to a disbalance in normal vaginal flora. It is more commonly present in females of the age group (15-44) and is the most common cause of pre-term labor, post-cesarean complication, and postpartum endometritis (infection of the lining of the uterus).
It is called vaginosis instead of vaginitis because the normal lactobacillus is replaced by anaerobes or other organisms. These anaerobes produce proteolytic carboxylase which causes vaginal secretions and exfoliation of squamous epithelial cells.
Clinical Syndromes of bacterial vaginosis
The clinical syndromes of bacterial vaginosis include:
Malodorous white vaginal secretions absorb into the vaginal wall
fishy odor by the addition of 10% KOH in vaginal secretion called Whiff’s test
presence of “clue cells” i.e. epithelial cells surrounded by coccobacillus organism
pH >= 5, the presence of all or at least 3 symptoms indicates bacterial vaginosis
Common organisms associated with bacterial vaginosis - Gardnerella vaginalis, Mycoplasma hominis
Laboratory diagnosis for Gardnerella vaginalis
The laboratory diagnosis for Gardnerella vaginalis starts with the collection of samples.
Sample
vaginal swab, vaginal discharge, endocervical swab
*specimen is transported in the Stuart medium
Microscopy
gram staining of the smear shows Gram-variable small bacilli and the presence of clue cells. These clue cells are the vaginal epithelial cells covered with many small gram-variable rods.
.jpg)
Fig: G. vaginalis gram-stain (Source: Wikipedia)
Culture
inoculated on (BA) Human blood polysorbate so medium which contains colistin, nalidixic acid, and amphotericin D that makes it selective for Gardnerella vaginalis
incubated at 5% CO2 at 33-37°C for 48 hours
the colonies are small, opaque colonies with distinct β-hemolysis
Identification by Gram staining, coagulase-negative, and positive hippurate hydrolysis test
Confirmatory identification
gram stain => gram variable cocco-bacilli
diffuse β-hemolysis
Catalase negative, Oxidase negative
Fructose, Galactose, Glucose, Mannose and ribose fermenter
Zone of Inhibition (ZOI) in AST =>Meteronidiazole (50 micrograms)
Trimethoprim and sulphamide
Other tests
To differentiate the infection of G. vaginalis, from Trichomonas and Candida albicans, numerous tests are used including the amine whiff test. In this test, 10% KOH is added to the discharge. If the fishy smell is produced, then the etiological agent is G. vaginalis.
AST
sensitive to penicillin, ampicillin, and trimethoprim
resistant to gentamicin, nalidix acid and colistin
Metronidazole, Clindamycin is the drug of choice - can be administered orally or as vaginal gel/cream
Laboratory diagnosis for Mycoplasma hominis
The laboratory diagnosis for Mycoplasma hominis includes:
Sample
Genital secretions/swabs
joint fluids
amniotic fluid
blood
pleural secretions
urine
tissue and wound aspirates
* For isolation of M. hominis, the sample is pre-enriched in Mycoplasma broth (contains arginine and urea). It also contains 10 micrograms/ml of erythromycin which makes it selective for M. hominis.
Transport
Since mycoplasmas do not have a cell wall, they are highly susceptible to drying. Thus, transport media is required in cases of delayed examination. Suitable transport media such as SP4 transport medium can be used to prevent desiccation
If the storage time is expected to exceed 24 hours prior to cultivation, the sample + transport medium should be frozen at -80°C.
Microscopy
cell-wall deficient so the gram stain is poorly observed- hence not done
Acridine orange or fluorochrome stain can be used. But they are non-specific stains and will stain other bacteria as well as human cells with nucleic acid
Direct Ag-detection
Direct/Indirect immunofluorescence
Counter-current immunoelectrophoresis
Immunoblotting
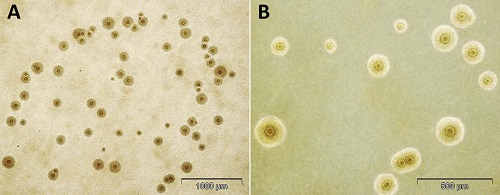
Fig: M. hominis colony (Source: Urology Gold Journal)
Culture
* Due to its fastidious nature and slow growth (3-4 weeks), culture is not generally done in routine diagnosis.
However, it can be cultured in selective media to prevent the overgrowth of faster-growing organisms and is incorporated with Urea or arginine. If color change is observed (pH change), a 0.1-0.2ml aliquot is subcultured to fresh broth or agar media.
After enrichment, it is transferred in A8 agar and incubated in an atmosphere of 95% N2 and 5% CO2 at 35-37°C for 24-48 hours. Fried egg colonies are observed on A8 media which are 20-300 micrometers in diameter.
Media used are => A7 and A8 agar medium; Triphasic system (Modified) NYC medium; shepherds 10B broth SP4 glucose broth with arginine or urea.
Identification of bacteria
Agar is examined at 24-72 hrs following incubation
M. hominis colonies are large (20-300 micrometers in diameter) and are urease negative with a fried-egg appearance
On BA, it produces non-hemolytic, pinpoints colonies that do not stain with gram’s stain but do stain with Dienes or acridine orange stains.
Serodiagnosis
CFT
ELISA
EIA
Indirect immunofluorescent Ab test
Indirect hemagglutination (rarely used)
Metabolism inhibition (rarely used)
Confirmatory test
Growth inhibition by homologous antisera
Molecular diagnosis- PCR
AST, Therapy
Resistant to erythromycin and occasionally to tetracyclines. In such cases, clindamycin is used in treatment.