Coxiella burnetii - Cell wall, Antigen, Pathogenesis, Lab Diagnosis, AST, Therapy, Prevention
Cell wall components, Antigenic structure of Coxiella burnetii
Cell wall components and antigenic structure of Coxiella burnetii bacterium exist in two forms:
phase 1 Ag
phase 2 Ag
Phase 1 Ag
phase 1 Ag is a cell wall LPS Ag with a complex carbohydrate structure
It prevents the interaction of Ab with surface protein
highly infectious
highly immunogenic and elicits a strong Ab response to both 1 and 2 Ag
Phase 2 Ag
This occurs by following repeated passage in the yolk sac in which LPS is modified by exposing the surface proteins to Ab
In phase 2 Ag, surface proteins act with the host Ab
less infective form
The acute stage of Q fever is characterized by the presence of Ab titers against phase 2 Ag. The chronic stage of Q fever is characterized by the presence of Ab titers against both phase 1 and phase 1 Ag.
Pathogenesis of Coxiella burnetii
Coxiella burnetti causes infection by penetrating through abraded skin, mucosa, lung, or intestinal tract. Following infection, it is phagocytized by the host cell and multiplies in an acidic environment of phagosome and lysosome
The IP is about 2 weeks to 1 month
After infection and proliferation in the lungs, they are picked up by macrophages and carried to the lymph nodes, from which they then reach the bloodstream
Phase 1 form is protected from the action of antibiotics. They affect the lungs and heart valves. It also causes granulomatous changes in reticuloendothelial organs such as the liver, spleen, etc.
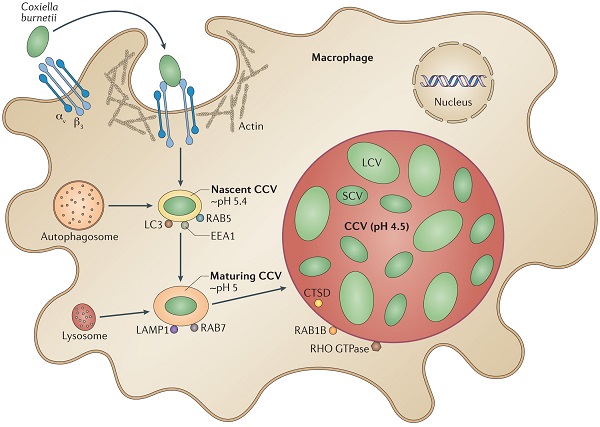
Coxiella burnetti in a host cell (Image: Nature)
Laboratory Diagnosis of Coxiella burnetii
The laboratory diagnosis of Coxiella burnetii is mostly based on serological tests.
Serodiagnosis
serodiagnosis is the most convenient and commonly used laboratory diagnosis method for Coxiella burnetii
IFA, ELISA, and CFT used
these tests detect IgM and IgG Ab by using phase 1 and phase 2 Ag
the Weil-Felix test is not used
Serodiagnosis of acute Q fever is made by demonstration of
IgM titer of 1:200 or more or IgM titer of 1:50 or more in a single serum sample
Fourhold rise in Ab titer between acute and convalescent sera:
* IgG Ab is present in serum for more than one-year-old
* IgM Ab is present in serum only for two weeks
* Ab against phase 1 Ag is always higher
Molecular diagnosis
PCR is the most commonly used molecular method for the diagnosis of Coxiella burnetii.
AST, Therapy of Coxiella burnetii
AST is not usually performed as it cannot grow in bacteriologic culture media
Tetracycline for both acute and chronic Q fever
Prevention of Coxiella burnetii
vaccine is available