Pneumocystis jirovecii - Complication, Prognosis, Laboratory Diagnosis, Epidemiology, Reservoir, Transmission, Treatment
Complications of Pneumocystis jirovecii
In rare cases (less than 3%) complications may occur, Pneumocystis jirovecii may disseminate and form extra-pulmonary lesions. Spleen, liver, bone marrow, and lymph nodes may be involved in such cases.
Prognosis of Pneumocystis jirovecii
In case Pneumocystis jirovecii pneumonia (PCP) is untreated, the prognosis is poor as pulmonary damage may lead to death.
Epidemiology of Pneumocystis jirovecii
Epidemiologically, Pneumocystis jirovecii is distributed worldwide- in both humans and animals. Animal hosts include mostly mammals such as sheep, goats, horses, monkeys, guinea pigs, chimpanzees, mice, rats, and rabbits.
Geographically, the fungi have been reported in China, Japan, Iran, Israel, South America, Congo, USA, Canada, Brazil, Australia, Malaysia, New Zealand, and Euro-Asia.
Reservoir, Source of Pneumocystis jirovecii
Infected man or any animal is the main source and reservoir of infection for Pneumocystis jirovecii. A mature cyst is believed to be the infective form of this fungi.
Transmission of Pneumocystis jirovecii
Transmission of Pneumocystis jirovecii takes place by:
Man-to-man transmission
since it is an air-borne infection, inhalation of mature cysts via aerosols transmits the infection
congenital transmission
maybe caused by Pneumocystis jirovecii infection but is rare
Laboratory diagnosis of Pneumocystis jirovecii
The laboratory diagnosis of Pneumocystis jirovecii begins with the collection of samples:
Sample
Bronchoalveolar lavage (BAL)
sputum
lung biopsy
transbronchial biopsy
Microscopy
Microscopy is done to demonstrate the presence of Pneumocystis jirovecii in the specimen.
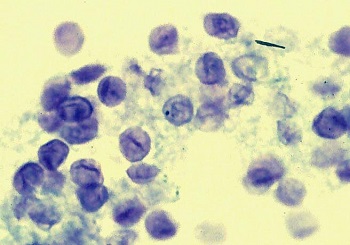
Figure: Pneumocystis jirovecii Toluidine Blue O stained cyst (Source: SciELO)
Staining microscopy
Stains such as Giemsa, polychrome methylene blue, methylamine silver, toluidine blue O, and Gram-Weigert stains are used.
Giemsa and polychrome methylene blue are unreliable as they also stain host tissue sections and may be difficult to interpret
methylamine silver, toluidine blue O, and Gram-Weigert stains only stain the cell wall of Pneumocystis jirovecii and hence are more reliable
* However, these stains also stain fungi but not the internal contents of Pneumocystis jirovecii cysts
Since all the above stains cannot differentiate antigenic variants of the fungi, the procedure lack sensitivity.
Immunofluorescence (IF) methods
it uses monoclonal antibodies
higher sensitivity than conventional microscopy
Serodiagnosis
serodiagnostic tests that can be used to diagnose Pneumocystis jirovecii infection include
Complement Fixation Test (CFT)
Indirect Fluorescent Antibody (IFA)
Enzyme-Linked Immunosorbent Assay (ELISA)
Western Blot
Counter-current immunoelectrophoresis (CIEP)
Latex Agglutination Test (LAT)
uses whole fungi or soluble extracts of fungi as antigens
does not differentiate between previous and active infection
can cross-react with Toxoplasma gondii
Molecular diagnosis
The molecular diagnosis of Pneumocystis jirovecii can be done by following methods:
DNA hybridization
in situ rRNA hybridization
PCR
Other methods
Imaging methods – chest X-ray
pulmonary function

Image: Pneumocystis jirovecii X-ray (Source: Radiopaedia)
Treatment of Pneumocystis jirovecii
Treatment of Pneumocystis jirovecii is done by supportive therapy and specific therapy.
Supportive therapy
aeration by a high concentration of oxygen, blood transfusion, etc
Specific chemotherapy
Trimethoprim-sulfamethoxazole
pentamidine
trimetrexate and folinic acid
primaquine and clinamycin
dapsone
Prevention, Control of Pneumocystis jirovecii
Prevention and control of Pneumocystis jirovecii infection can be done by the use of medical-grade masks by immunodeficient individuals.
Populations at risk of infection include:
premature and/or malnourished infants
children with primary immunodeficiency
people with protein malnutrition
individuals under treatment including immunosuppressive drugs such as corticosteroids for malignancy, organ transplantation, etc
HIV/AIDS patients