Dracunculus medinensis - Complications, Prognosis, Epidemiology, Reservoir, Source, Transmission, Lab diagnosis, Treatment, Prevention, Control
Complications of Dracunculus medinensis
The most serious complication of Dracunculus medinensis is a secondary bacterial infection at the site of the ulcer. If the gravid female parasite breaks during attempts of extracting the parasite, the larvae may remain inside the sub-cutaneous tissue resulting in cellulitis and abscesses.
Other complications include tetanus, arthritis, chronic ulcers, fibrosed joints, etc.
Prognosis of Dracunculus medinensis
The prognosis of Dracunculus medinensis infection is good with surgical removal of the parasite after using local anesthesia.
Epidemiology of Dracunculus medinensis
Epidemiological studies have shown that Dracunculus medinensis is prevalent in 18 countries and is widespread in Africa. The parasitic infection has been recorded in African countries including West Africa, Kenya, Uganda, Sudan, and Middle Eastern countries like Iran, Yemen, and Saudi Arabia.
Reservoir, Source of Dracunculus medinensis
Humans are the only reservoir of Dracunculus medinensis infection. Although animals such as dogs, cats, and foxes are found to be infected with Dracunculus medinensis, they do not constitute a reservoir.
The source of the parasitic infection is water infested with infected cyclops (twelve species including Mesocyclops leuckarti, Mesocyclops hyalinus).
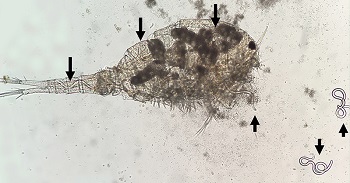
cyclops infected with L3 larvae of Dracunculus medinensis (black arrow) (Source: capcvet.org)
Transmission of Dracunculus medinensis
Transmission of Dracunculus medinensis occurs after drinking water contaminated with cyclops harboring the infective third-stage larvae of Dracunculus medinensis.
Laboratory diagnosis of Dracunculus medinensis
Laboratory diagnosis of Dracunculus medinensis is done by microscopic demonstration of first-stage larvae in the discharge fluid of the blisters. Adult parasites can be observed on the site of ulceration.
Sample
discharge fluid (from blisters)
Microscopy
Microscopy of discharge fluid (from blisters) is done by direct wet mount microscopy.
Direct Wet Mount
Direct wet mount microscopy of Dracunculus medinensis involves using 2 to 3 drops of discharge fluid sample on a clean glass slide and examination under a microscope.
The presence of live microfilariae, characterized by tadpole-like movement, confirms the diagnosis.

third-stage Dracunculus medinensis microfilariae (Source: ResearchGate)
Serological methods
The serological methods include tests for the demonstration of circulating antibodies in the specimen. Some commonly used serological methods are:
indirect fluorescent antibody (IFA)
indirect haemagglutination (IHA)
enzyme-linked immunosorbent assay (ELISA)
Western blot
Imaging methods
use of X-ray on infected areas shows dead or calcified parasites
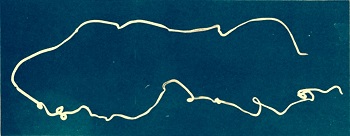
female Dracunculus medinensis (Source: Labweeks)
Treatment of Dracunculus medinensis
Although no specific drugs are available to use against Dracunculus medinensis, Thiabendazole, and Metronidazole are used to enable the rapid emergence of worms and quick healing of ulcers.
Antibiotics and anti-inflammatory drugs are administered in case of secondary infections.
Surgical removal of the parasite under local anesthesia, while taking care not to break it, is done as treatment.
Prevention, Control of Dracunculus medinensis
Prevention, Control of Dracunculus medinensis is done by following steps:
successful treatment of infected individuals
reduction of transmission by consumption of only safe drinking water (filtered, boiled)
improvement of sanitation and personal hygiene