Onchocerca volvulus - Epidemiology, Reservoir, Transmission, Laboratory diagnosis, Treatment
Epidemiology of Onchocerca volvulus
Epidemiological studies of Onchocerca volvulus have revealed 17–25 million people infected with Onchocerca volvulus and 0.8 million showing some impairment of vision due to the filarial nematode. It is estimated that 187 million people are at risk of infection. Although the parasite has not been recorded as a cause of a single death, it is the major cause of disability.
About 99% of Onchocerca volvulus infections occur in 31 countries in sub-Saharan Africa while in Latin America (Brazil, Venezuela,), the disease is believed to have been brought by the slave trade.
The infection rate is high along the banks of rivers in the rainforests as well as in Savannah areas.
Reservoir, Source of Onchocerca volvulus
Infected humans are the only source and reservoir of Onchocerca volvulus infection as it lacks any animal reservoir.
Transmission of Onchocerca volvulus
Transmission of Onchocerca volvulus occurs via the bite of infected female black flies of the genus Simulium during a blood meal.
Laboratory diagnosis of Onchocerca volvulus
The laboratory diagnosis of Onchocerca volvulus is done by demonstration of microfilariae in the skin snips.
Sample
skin snips
* skin snips from buttocks, iliac crests, leg calves (Africa)
* skin snip from behind shoulders, truck (Mexico)
* skin snip from lower limbs (Yemen)
skin scratches
biopsy tissue (from sub-cutaneous nodule)

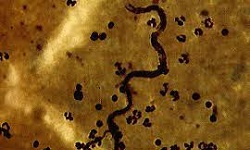
Onchocerca volvulus microfilariae (Source: World Federation of Parasitologists)
Microscopy
Microscopy of the skin snip specimen to observe the presence/absence of microfilariae is done.
Bloodless skin snips are collected with the help of a sterile needle and a razor blade.
Procedure of skin snip:
around 3mm of skin is raised with the tip of a needle and cut off with a sterile razor blade
skin snip is placed on a slide or in the well of a microtitration plate
the specimen is immersed in the physiological saline and left at room temperature for 30 to 60 minutes
* during this time, Onchocerca volvulus microfilariae emerge out of the skin into the saline
the slide is examined under a microscope for the presence/absence of microfilariae
if microfilariae are not seen, the slide is left overnight and re-examined
This method is specific and accurate but cannot differentiate between early or mild infections.
Skin scratch samples are obtained by careful removal/scrapping of the superficial layer of the epidermis with the blunt edge of the disposable lancet.
Serodiagnosis
If Onchocerca volvulus microfilariae are not observed in skin snip microscopy, serological tests can be used for serodiagnosis. However, a major disadvantage is that it cannot differentiate between past and present infections.
Some serological tests used include:
ELISA (uses microfilarial antigens)
rapid-format antibody card test (uses Ov16 antigen to detect immunoglobulin G4)
Molecular methods
PCR is the most common molecular method for the diagnosis of Onchocerca volvulus. This test can also detect the migration of microfilariae back to the host skin following treatment.
Imaging Methods
Ultrasound can detect vitreous changes in the eyes as well as deep onchocercoma.
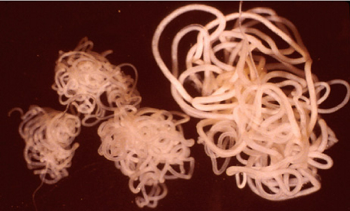
Onchocerca volvulus - three adult males, one adult female(Source: ResearchGate)
Other tests
Other tests for diagnosis of Onchocerca volvulus include:
histological diagnosis – demonstration of adult worms in the biopsy tissue from subcutaneous nodule
slit-lamp examination – if present, live microfilariae is observed on the cornea
DEC patch test – also known as Mazzotti patch test which is specific but less sensitive
* DEC patch produces a local reaction to dead microfilariae at the patch site
Treatment of Onchocerca volvulus
Onchocerca volvulus is treated by oral administration of Diethyal carbamazepine (DEC), and Ivermectin.
Surgical removal of nodules is also done.