Plasmodium vivax - Clinical Manifestation, Prognosis, Epidemiology, Reservoir, Transmission, Control, Treatment
Clinical Manifestation of Plasmodium vivax
The incubation period of malaria by Plasmodium vivax is 8 days to 31 days. Although they cause the most widespread malaria, they are less severe than P. falciparum, and death from Plasmodium vivax is less common.
Malaria paroxysm
shivering and cold followed by fever which can last from 2 hours to 6 hours
fever can reach as high as 40.6°C (105°F)
other symptoms accompanying fever include dry skin, headaches, nausea, and vomiting
finally, the fever subsides with the patient sweating heavily
Malarial fever
caused by rupture of mature schizonts from the infected host liver cells
In cases infected by Plasmodium vivax and P. ovale, schizonts are released every 48 hours, thus malaria fever occurs every 48 hours
enlarged spleen and anemia are also associated with children
Relapse
feature of Plasmodium vivax infection
caused by the activation of hypnozoites in the liver cells
the relapse rate is at 50% within 5 weeks (short-term relapse) or 5 years (long-term relapse) from the initial syndrome
the type of relapse depends upon the strain of Plasmodium vivax infecting the individual
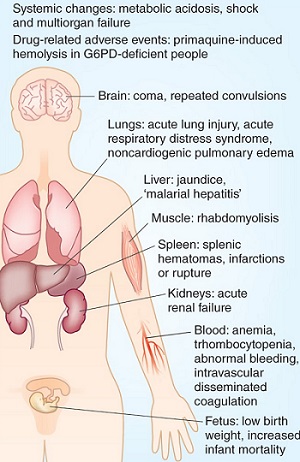
Figure: malaria clinical manifestation (Source: nature)
Complication of Plasmodium vivax
In cases of a ruptured spleen, which has been enlarged due to malaria infection, it may be life-threatening
Prognosis of Plasmodium vivax
The Plasmodium vivax malaria infection is treatable with the administration of anti-malarial drugs.
Epidemiology of Plasmodium vivax
Plasmodium vivax is widely distributed- even more than P. falciparum. However, they have low morbidity and mortality.
The occurrence of Plasmodium vivax is more common in temperate countries than in tropical countries.
Geographically, they are found in South America, Australia, tropical and subtropical Africa, Northern Africa, China, Korea, USSR, Pakistan, Sri Lanka, Bangladesh, India, etc.
Reservoir, Source, Transmission of Plasmodium vivax
Man is the only source and reservoir of the Plasmodium vivax.
Transmission occurs during the blood meal by sporozoite-infected female Anopheles mosquitoes. The congenital transmission also occurs in cases of Plasmodium vivax.
Prevention, Control of Plasmodium vivax
The prevention and control of Plasmodium vivax infection are based on
successful treatment of infected individuals
reduction of transmission by controlling mosquito population especially around housing by eliminating breeding places, spraying oils and chemicals in breeding sites
using mosquito nets while sleeping, and netted windows in endemic areas
wearing protective clothing
use of mosquito repellants
chemoprophylaxis
Treatment of Plasmodium vivax
Chloroquine (for the erythrocytic stage), primaquine (for the liver stage of the parasite), fanasil (sulphorthodimethoxine), and mefloquine are the drugs of choice
in recent years, resistance to primaquine has been reported and hence large doses are used in some parts of Asia and New Guinea