Toxoplasma gondii - Life Cycle, Pathogenesis, Pathology, Host Immunity
Life Cycle of Toxoplasma gondii
The life cycle of Toxoplasma gondii completes in the definitive host and intermediate host.
Definitive host: cats and other felines are the definite hosts and asexual cycle of the parasite.
Intermediate host: takes place in warm-blooded animals such as birds and mammals (man, goat, sheep, pig, cattle, etc)
Asexual cycle
The asexual cycle or extra-intestinal cycle takes place in man, non-felines, birds, and other mammals
infection in humans begins with the ingestion of water and food contaminated with sporulating oocysts or tissue cysts present in raw or undercooked meat of another intermediate host such as mutton, pork, beef
once in the intestine, sporozoites from the oocysts and bradyzoites from tissue cysts invade the intestinal mucosa
in the host intestinal epithelial cells, undergo multiplication by endodyogeny to form trophozoites
* endodyogeny involves the formation of two progeny within the parent parasite which are released after the parent parasite disintegrates
the trophozoites continue to divide inside the host cells
these trophozoites may spread locally to mesenteric lymph nodes by invading new host cells or invades blood and lymphatics to distant extra-intestinal organs such as the brain, eye, liver, spleen, heart, skeletal muscle, and placenta of a pregnant mother
in the intestinal, mesenteric, and in extra-intestinal organs, the focal areas of necrosis develops
in about 30 weeks after infection, host immunity is able to destroy tachyzoites present in visceral organs and acute toxoplasmosis is resolved
however, some Toxoplasma gondii persist and continue to develop into large tissue cysts in the brain, skeletal muscles, or heart muscles
the tissue cysts which contain hundreds of bradyzoites remain viable for years which has a potential for re-activation
if immunosuppression occurs in the host, reactivation of the cyst may result in infection
since cattle are consumed and humans are not, the infection in man is a dead end
rats mostly acquire Toxoplasma gondii infection after preying on mice
Sexual cycle
The sexual or intestinal cycle takes place in the gastrointestinal tract of the definitive hosts such as cats and other felines
cats are infected with Toxoplasma gondii after consuming muscles, brain, and other tissues of prey animals (such as mice, and rats) or feeding on raw meat of domestic animals harboring the parasite tissue cysts
in the small intestine, the tissue cysts rupture to release bradyzoites which penetrate the mucosal epithelial cells of the small intestine
in the epithelial cells, they undergo several cycles of asexual generation followed by the sexual cycle
at the end of the sexual cycle, fertilized microgamete or zygote is formed by the fusion of bradyzoites
the zygote develops into an oocyst after being surrounded by a thin but rigid wall
the infected host cells rupture and oocysts are then released into the lumen of the intestine which is excreted in the cat feces for a period of 1-3 weeks
these unsporulated oocysts are not yet infectious but in the environment, they mature to form for up to 21 days
oocyst maturation, called sporogony, involves the formation of two sporocysts with each containing four sporozoites
infectious sporulating oocysts are hardy and can remain viable for more than one year in warm and humid environments
if man, birds, or other mammals ingest these sporulating oocysts, new hosts are infected and the life cycle of Toxoplasma gondii is continued
an extra-intestinal cycle of Toxoplasma gondii, which is mostly seen in intermediate hosts, is also seen in cats- possibly due to direct invasion of the lymphatic system or lymph nodes by tachyzoites from its own intestine
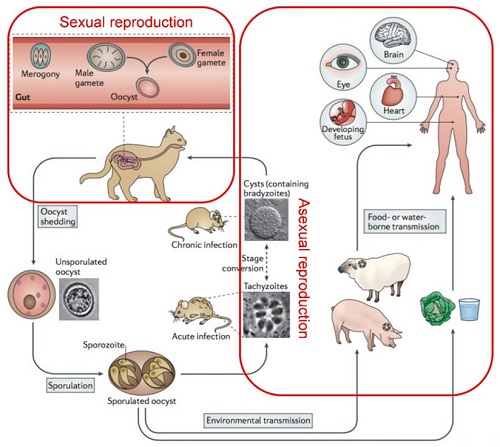
Figure: Toxoplasma gondii life cycle (Source: CDC)
Pathogenesis, Pathology of Toxoplasma gondii
In cases of acute infection, tachyzoites multiply in the gastro-intestinal and the extra-intestinal organs such as the brain, eye, liver, spleen, heart, skeletal muscle, and placenta of a pregnant mother
the parasites cause disruption and death of cells at these sites resulting in necrotic foci surrounded by necrotic foci
In cases of Toxoplasma gondii infection in an immunodeficient host, the acute infection may progress to result in potentially lethal conditions such as acute necrotizing encephalitis, myocarditis, and pneumonitis
the cyst can be found in host organs as early as 7 days from infection with each cyst containing anywhere between 50 to 3000 strongly PAS-positive bradyzoites
they are formed intracellularly inside the vacuoles and the wall surrounding the cyst is eosinophilic, argyrophilic, and weakly PAS-positive.
chronic Toxoplasma gondii is characterized by the presence of these cysts throughout the life of the host with little or no inflammatory response but the potential for reactivation
reactivation is much more common in immunocompromised, patients with chorioretinitis, or in children who have acquired the infection congenitally
Host Immunity of Toxoplasma gondii
Host immune response- both humoral and cell-mediated has significant responsibility for the course of infection and clinical manifestations caused by Toxoplasma gondii.
The development of both humoral and cell-mediated immunity in an immunocompetent host affects the outcome of acute toxoplasmosis. It is associated with the disappearance of tachyzoites from various tissues – especially from the extra-neural tissues and the formation of tissue cysts. However, due to the absence of circulating antibodies in the tissues, the tachyzoites may remain in the central nervous system and the eye.
Humoral immunity
characterized by the production of circulating antibodies including IgM and IgG
IgM is the first to appear and its detection is suggestive of acute infection
IgG antibodies appear later in infection and are indicative of chronic toxoplasmosis
Cell-mediated immunity
Cell-mediated immunity involves the activation of macrophages and monocytes
plays an important role in conferring resistance to re-infection
along with humoral immunity also helps in the development of initial resistance
In congenital toxoplasmosis
the immunological features of congenital toxoplasmosis include:
glomerulonephritis with deposits of IgM, toxoplasma antigen
decreased serum IgA
monoclonal gammopathy of IgG
circulating immune complexes in the serum
presence of Toxoplasma gondii-specific IgM antibodies
In acquired toxoplasmosis
in patients with lymphadenopathy and fever, immunological changes such as lymphocytosis, alternations in T lymphocyte subpopulations, increase in suppressor T-cell levels, and decrease in helper-to-suppressor T-cell ratio, occurs
in patients with only lymphadenopathy, a reduction in the number of helper cells for more than 6 months after the infection is seen
in AIDS patients, a significant decrease of inducer T-lymphocytes can be observed which may lead to severe manifestations observed in Toxoplasma gondii infection