Acanthamoeba - Clinical Manifestations, Lab diagnosis, Treatment
Clinical Manifestations of Acanthamoeba
As most Granulomatous amebic encephalitis (GAE) is fatal, the prognosis for Acanthamoeba is very poor. One of the complications may include cardiopulmonary arrest.
Granulomatous amebic encephalitis (GAE)
rare and chronic infection of the central nervous system
usually, infection is seen in immunocompromised individuals (AIDS, undergoing immunosuppressive therapy) or people who are malnourished, chronically ill, or debilitated
clinical symptoms for Acanthamoeba include low-grade fever, stiff neck, headache, and changes in mental status
neurologic symptoms are focal seizures, cranial nerve palsies, hemiparesis, aphasias, ataxias, or photophobia
as the disease progress from one week to several weeks, the patient may go into a coma
death may result from bronchopneumonia, kidney, and liver failures.
Acanthamoeba keratitis
it is a chronic, progressive, ulcerative infection of the eye that shows characteristic annular infiltration and congested conjunctiva
occurs in healthy individuals who commonly use contact lenses or have undergone recent trauma to the cornea
infection initiates with exposure to water contaminated with Acanthamoeba cysts or trophozoites
if not treated, the infection will progress to corneal perforation, blindness, and ultimately loss of the eye

Image: Acanthamoeba keratitis (Source: Eye Wiki)
Cutaneous lesions
it is common in disseminated cases of Acanthamoeba infections
appear after primary inoculation
lesions occur on the face, trunk, and extremities and start with erythematous nodules and indurated papules which suppurate and form ulcers. The nodules and papules are 1.5 cm to 3 cm in diameter while the ulcers are much larger
Laboratory diagnosis of Acanthamoeba
Since GAE is rarely diagnosed before death, Acanthamoeba diagnosis occurs post-mortem or shortly before death.
Sample
The samples collected for Acanthamoeba
brain biopsy
corneal lesion scrappings
CSF
Microscopy
demonstration of Acanthamoeba cysts and trophozoites in brain biopsy, CSF confirms GAE (75% of cases)
Acanthamoeba keratitis is confirmed by observation of morphological forms of the parasite in the corneal lesion during wet mount microscopy.
Acridine orange, Giemsa, LPCB, and Parker ink KOH stains are used to stain cysts and trophozoites
other methods to visualize cysts and trophozoites include immunofluorescence by fluorescence-conjugated lectins (concanavalin A) and wheat germ agglutin
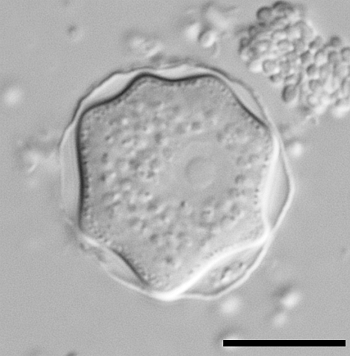
Image: Acanthamoeba electron microscopy (Source: Wikimedia commons)
Culture
Acanthamoeba culture can be done in
Non-nutrient agar inoculated with Page’s solution containing monoxenic culture of bacteria such as Enterobacter species, Aebacter aerogenes, and Escherichia coli
Axenic culture – enriched broth without added bacteria
monolayer cell lines cultures such as Hela cells, MRChuan embryonic lung cells, and monkey kidney cells
grows best at 25° C - 30° C
Serodiagnosis
The serodiagnostic approach for Acanthamoeba is not usually taken due to less sensitivity and specificity
Imaging Methods
A CT scan for Acanthamoeba may present multiple lucent, non-enhancing lesions in the infected brain cortex while focal lesions are seen throughout the CNS
Treatment of Acanthamoeba
not an effective treatment for GAE but Acanthomeoba keratitis has been successfully treated
for other forms of the disease, sulphonamides, clotrimazole, and polymyxin B can be used
other medications include topical miconazole, diamines such as propioaminide, dibromonpho amidine and antibiotics