Ancylostoma duodenale - Laboratory Diagnosis, Epidemiology, Reservoir, Transmission, Treatment
Laboratory diagnosis of Ancylostoma duodenale
Infection by the hookworm parasite Ancylostoma duodenale is difficult to diagnose in the laboratory. Conditions associated with the infection such as eosinophilic leucocytosis and hypochromic microcytic anaemia are linked to the parasite infestation in endemic areas.
Sample
The samples collected for the diagnosis of Ancylostoma duodenale include:
stool
lung biopsy/autopsy
Microscopy
Microscopy of stool is done to demonstrate the Ancylostoma duodenale eggs. However, as the eggs of Ancylostoma duodenale and Necator americanus are similar in morphology, misidentification may occur.
Stool microscopy
Among numerous stool microscopy methods, direct wet mount microscopy is done for the diagnosis of Ancylostoma duodenale.
Direct wet mount microscopy
the wet mount for Ancylostoma duodenale is prepared by mixing stool sample with saline, iodine, or lactophenol cotton blue (LPCB)
ancylostomiasis is confirmed by the demonstration of the hookworm eggs
adequate for the detection of moderate or severe infections i.e. around 1200 eggs/ml of faeces
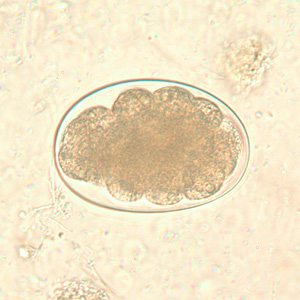
Ancylostoma duodenale egg (Source: ResearchGate)
Stool concentration
the formalin-ether method or salt flotation of stool is used for the concentration of the specimen for the detection of eggs of Ancylostoma duodenale
for quantitative diagnosis, egg counting technique such as Kato-Katz method is used as the load of parasites is directly associated with the severity of infections
Culture
The stool specimen is cultured by Harada Mori method to demonstrate the infective filariform larva (third-stage larva) which has hatched out of hookworm eggs present in the stool. It is done by smearing stool on moist filter paper and incubating it for 5 days to 7 days at room temperature.
This method has more advantages to stool microscopy as Ancylostoma duodenale and Necator americanus can be distinguished by the presence of infective filariform larva of Ancylostoma duodenale.
However, the stool specimen should be processed as soon as possible. If allowed to stand for several hours, the rhadbitiform larva that has hatched may be confused with Strongyloides.

Rhabditiform larva of Ancylostoma duodenale after wet mount preparation (Source: ResearchGate)
Other methods
X-ray of the chest for diagnosis of respiratory manifestation of the hookworm infections
Epidemiology of Ancylostoma duodenale
Infection by hookworm, both Ancylostoma duodenale and Necator americanus, are the second most common helminthic parasitic infection – ascariasis being the first.
Although the parasite is found to be worldwide, they are most common in areas with warm and moist climates – throughout the tropics and subtropics. Incidence is high in places where people defecate in the open ground, in rural areas, and in children.
Reservoir, Source of Ancylostoma duodenale
Human faeces is the only source of infection as well as the reservoir for Ancylostoma duodenale infection.
Transmission of Ancylostoma duodenale
Ancylostoma duodenale is transmitted by the following methods:
cutaneous route – penetration of host skin by filariform larvae. Common sites include feet, hands, buttocks or areas frequently exposed to soil
oral route – ingestion of filariform larvae. A less common route of infection
trans-mammary route – from breast milk. Rare route of infection
transplacental transmission
Treatment of Ancylostoma duodenale
Treatment of Ancylostoma duodenale infection is done by administration of anthelmintics (eg. mebendazole) as well as iron replacement therapy in cases of iron deficiency anaemia (severe anaemia).
Prevention, Control of Ancylostoma duodenale
Prevention, and control of Ancylostoma duodenale are done by:
Individual prophylaxis
Individual prophylaxis of Ancylostoma duodenale is done by
improved personal hygiene such as proper washing of hands with soap after defecation and before eating food
treatment of water before drinking such as boiling, filtering the water used in a 0.22-micrometre membrane, iodination with tetracycline hydro per iodide
drinking bottled water while travelling to areas endemic to ancylostomiasis
if salad is to be consumed, treat the vegetables with acetic acid or vinegar for 15 minutes
not performing sexual acts that involve faecal-oral contact
Community prophylaxis
Community prophylaxis of Ancylostoma duodenaleis done by
improvement of the water management system to avoid faecal contamination
improvement of sanitation by installing latrines for proper disposal of human faeces