Ancylostoma duodenale - Life Cycle, Pathogenesis, Pathology
Life Cycle of Ancylostoma duodenale
The life cycle of Ancylostoma duodenale is completed in a single host i.e. humans. No intermediate hosts are required to complete its life cycle.
Infection by Ancylostoma duodenale begins with penetration by the filariform larva of the parasite, usually on the barefoot
after initially shedding their sheath, they use mechanical and lytic actions to travel into the dermis and subcutaneous tissues
Ancylostoma duodenale then enters the lymphatics and veins from which they reach the right heart and then to the lungs via host blood circulation
in the lungs, the parasite ruptures the capillaries to reach the alveolar spaces
from the alveolar spaces, the hookworm climbs the bronchial tree to the pharynx and then swallowed reach the small intestine
during the larval tour, in the oesophagus, the Ancylostoma duodenale larval undergo a third moult and becomes fourth-stage larvae (L4)
the L4 larvae have a buccal capsule which functions by adhering to the host intestinal wall
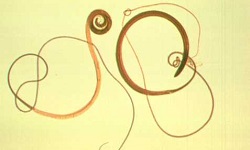
after one final stage of moulting, the hookworm develops into an adult which sexually matures within 4 weeks to 5 weeks
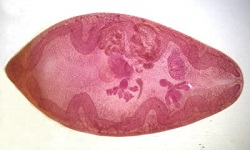
after mating, the female hookworm begins to lay fertilized unembryonated eggs which are released out in the faeces
the time between infection and release of eggs in the host faeces is 6 weeks
under favourable conditions (warm, damp, well-oxygenated soil), within 24 to 48 hours, the eggs hatch to release rhabditiform larvae (L1)
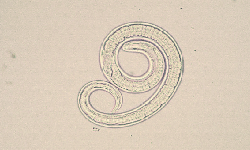
the rhabditiform larvae of Ancylostoma duodenale undergo two stages of moulting (on the third day and on the fifth day) and develop into filariform larvae (L3) in 5 to 8 days
the filariform larvae of Ancylostoma duodenale, which is the infective stage of the parasite, can live for 3 weeks to 4 weeks under favourable conditions
if the filariform larvae are able to penetrate the skin of the new host and cause infection, the life cycle is continued
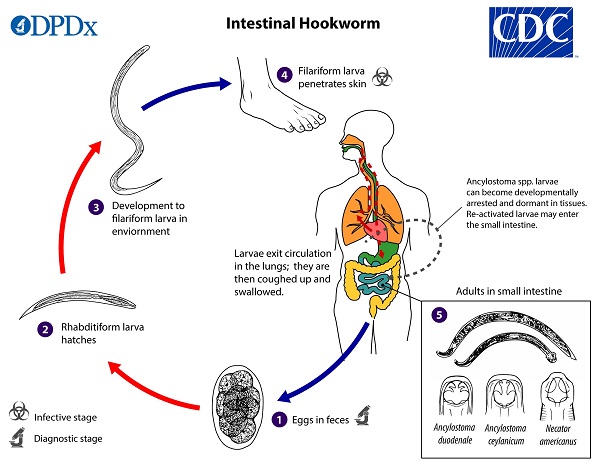
Lifecycle of Ancylostoma duodenale (Source: CDC)
Pathology of Ancylostoma duodenale
The pathology of Ancylostoma duodenale is caused mainly due to the presence of adult worms in the intestine. The penetration and migration of filariform larvae also cause pathological changes in infection caused by hookworm, although it is less frequent.
Pathogenesis of Ancylostoma duodenale
Pathogenesis by the adult worm
At the site of infection i.e. the upper small intestine, pathogenesis occurs due to the attachment of adult Ancylostoma duodenale onto the host intestine by buccal capsule. In cases of heavy infection, the parasites may be present as far as the lower ileum of the intestine.
The mouthparts of the parasite penetrate the blood vessels which suck blood for consumption. As a result, loss of blood and tissue fluids occurs i.e. 0.15ml to 0.26ml of blood per day per hookworm.
Adult hookworm causes blood loss in hosts which is a result of
ingestion of blood by the hookworm
seepage of blood from the site of attachment
loss of blood from the previously burrowed site
anticoagulants released by the buccal capsule prevent blood clotting at the wound site
Hypochromic microcytic anaemia, which is caused by heavy and prolonged infections, may become serious to fatal in individuals with low iron intake or absorption.
In cases where there is a loss of protein, oedema and hypoproteinaemia may occur.
Pathogenesis of infective larva
When infective filariform larvae penetrate the host skin, it produces ground itch which is an allergic manifestation. Secondary bacterial infections in sensitised hosts can cause serious complications.
If the migrating larvae through the host lung are large in number, they may produce haemorrhage and infiltration of leucocytes. As a result, larvae may be entrapped in the lung tissue and both eosinophilia and leucocytosis may occur at this stage.