Echinococcus granulosus - Laboratory Diagnosis, Treatment, Prevention, Control
Laboratory diagnosis of Echinococcus granulosus
The laboratory diagnosis of Echinococcus granulosus begins with collection of samples:
Sample
urine
sputum
hydatid fluid aspiration
Aspiration of Echinococcus granulosus hydatid fluid from an intact cyst in the lung has been attempted for diagnosis but this is not recommended because of the possibility of anaphylactic reactions if fluid leaks and the risk of secondary echinococcosis due to spillage of protoscolices from the viable cysts.
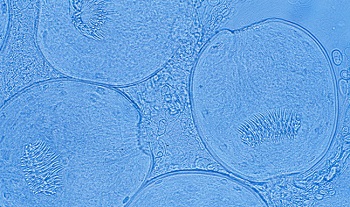
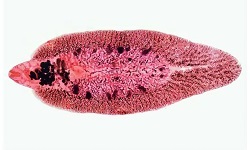
Image: E. granulosus cluster of Scoleces (Source: webpathology)
Microscopy
Microscopy of Echinococcus granulosus depends on the demonstration of brood capsules and protoscolices in hydatid fluid aspiration.
Direct Wet Mount Examination
the direct wet mount is prepared by mixing saline, and sometimes iodine or lactophenol cotton blue (LPCB) can be used
centrifuged hydatid fluid deposit may reveal protoscolices as colorless white structures
if lactophenol cotton blue (LPCB) is used for wet mount preparation, the protoscolices and scolices appear deep blue which helps in easy detection and identification
Acid Fast staining
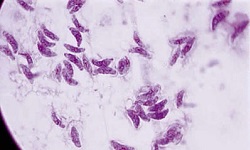
smears from centrifuged Echinococcus granulosus hydatid fluid deposit after acid-fast staining reveals purple or pink colored protoscolices and scolices

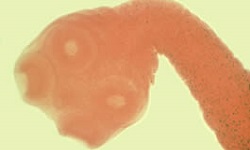
Image: E. granulosus cyst (Source: wikipedia)
Casonis’ skin test
Casonis’ skin test is an immunodiagnostic test based on an immediate hypersensitivity skin test. It is used in the diagnosis of cystic echinococcosis caused by Echinococcus granulosus.
However, due to low sensitivity (55%-75%) and low specificity, false positive reactions may occur in patients suffering from other cestode infections- limiting the value of this test
The procedure for the test:
inject 0.2ml of sterile hydatid fluid intradermally in one arm
* hydatid fluid is obtained from cysts in humans during surgery, from sheep during an autopsy, and sterilized by filtration
inject 0.2ml of sterile normal saline intradermally in another arm as a control
if a large wheal measuring 5cm or more in diameter with multiple pseudopodia is seen, it indicates a positive reaction

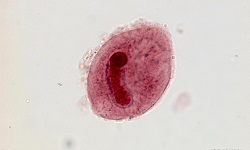
Image: E. granulosus adult (Source: wikipedia)
Serological test
Serological tests are used for the primary diagnosis of cystic echinococcosis (CE) due to Echinococcus granulosus infection. This test is based on the detection of specific hydatid antibodies present in the serum as well as hydatid antigens in the serum, urine, or other body fluids.
Detection of antibodies
Echinococcus granulosus antibodies, if developed in the host body, can be detected by the following methods:
Indirect haemagglutination (IHA)
immunoelectrophoresis-in-gel, counter-current immunoelectrophoresis (CIEP)
enzyme-linked immunosorbent assay (ELISA)
Western Blot
The antibody-based immunoassay tests have several disadvantages including
low sensitivity results in false negative as antibodies are not produced in 10% of cases and in 40% of cases where lungs and liver are involved while cysts in the brain produce no antibodies
low specificity as Captons’ arc 5 antigen shows cross-reactivity with sera from alveolar echinococcosis and neurocysticercosis
these tests cannot differentiate between old or recent infections as hydatid-specific antibodies remain in circulation for a longer time
Detection of antigen
Echinococcus granulosus antigen can be detected by the following methods:
bacterial Co-agglutination (Co-A) – in urine samples
immunoelectrophoresis-in-gel, counter-current immunoelectrophoresis (CIEP) – in urine samples
enzyme-linked immunosorbent assay (ELISA)
Latex agglutination test (LAT)
A major advantage of antigen detection methods is that can differentiate between old or recent infections as hydatid antigens disappear immediately after cure by surgery or chemotherapy.
Imaging methods
Echinococcus granulosus can also be diagnosed by imaging methods such as:
X-ray
Ultrasound
CT scan
MRI

Image: CT-scan of intracranial hydatid cyst (Source: webpathology)
Other tests
Other tests includes histopathological tests (Periodic acid-Schiff stain i.e. PAS stain, Fine-needle aspiration cytology i.e. FNAC)
Treatment of Echinococcus granulosus
The treatment of Echinococcus granulosus takes place by the following methods:
Surgery
surgery remains the main course of treatment for cystic echinococcosis (CE)
done if the site of infection is operatable – lungs, liver
performed if enlarged cysts are likely to interfere with viral organ functions
however, surgery is associated with morbidity, mortality (2%), and recurrence rate (2%-25%)
Chemotherapy
This chemotherapy process is followed if the Echinococcus granulosus cyst is small in size or situated in in-operable areas. Drugs of choice include albendazole and mebendazole.
Prevention, and Control of Echinococcus granulosus
To prevent and control Echinococcus granulosus infection, the following steps can be taken:
regular treatment of reservoir i.e. dogs
prevent dogs from eating raw offal of domestic animals- especially in slaughterhouses
good personal hygiene – washing hands after feeding or petting/touching the dog
proper disposal of dog feces
eating well-cooked food, vegetables or proper washing of fruits before consumption
drinking safe boiled water – especially in endemic areas