Giardia intestinalis - Clinical manifestations, Laboratory Diagnosis, Treatment, Prevention, Control
Clinical manifestations of Giardia intestinalis
The incubation period of Giardia intestinalis ranges from 1 to 3 weeks and the infection may remain asymptomatic in the majority of the cases. Symptoms are mostly seen in children and vary depending on whether it is acute or chronic. In adults malabsorption syndromes and weight loss occurs while in children growth retardation is seen.
Since giardiasis is self-limiting and only 5% of cases become chronic, the prognosis is good- although death may occur in severely malnourished children.
Acute giardiasis
Symptoms to describe acute giardiasis includes watery diarrhea, abdominal cramps, bloating, flatulence, and in rare cases, nausea, vomiting, fever, rash, or constipation is presented.
acute diarrhea, caused by Giardia intestinalis, is the most common symptom (90% of symptomatic cases) which starts with profuse watery stool which later changes to voluminous, foul-smelling, and greasy and lasts for 5 to 7 days
abdominal cramps, bloating, and flatulence occurs in 70%-75% of symptomatic cases
Chronic giardiasis
symptoms include chronic diarrhea with steatorrhoea (malabsorption of fat), weight loss, nausea, anorexia, malaise
malabsorption of other essential nutrients such as vitamin A, protein, and D-xylose is also seen
in children, external abnormalities such as protuberance of the abdomen, spindly extremities, and stunted growth are seen
in rare chronic cases, the infection may become extra-intestinal with manifestations such as urticaria and reactive arthritis
if left untreated, chronic giardiasis caused by Giardia intestinalis may last from a week to several months
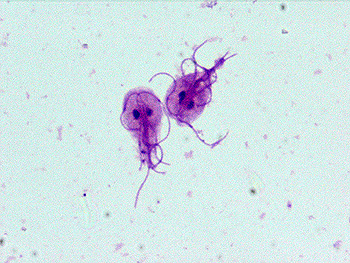
Image: G. lamblia trophozoites under a microscope (Source: Stepwards)
Laboratory Diagnosis of Giardia intestinalis
The laboratory diagnosis of Giardia intestinalis begins with the collection of specimens.
Specimen
The lab diagnosis of Giardia intestinalis includes a collection of specimens includes:
stool
bile-stained mucus
duodenal/jejunal biopsy
Microscopy
microscopy of stool samples is done to demonstrate the presence of Giardia intestinalis cysts or trophozoites.
* Cysts are usually present in the soft and formed stool while trophozoites are mostly present in the fresh watery stool.
after one stool examination, 50%-70% of stool with the parasitic cysts is detected and after three stool examinations, the sensitivity increases to 90%
stool microscopic examination includes
* Direct wet mount examination
* Stained stool smear examination
* examination of a stool after concentration
Direct wet mount microscopy
the wet mount for Giardia intestinalis is prepared by mixing stool sample with saline, iodine, or lactophenol cotton blue (LPCB)
giardiasis is confirmed by the demonstration of trophozoites which is identified by “falling leaf” motility
useful mostly in the detection of freshly passed diarrhoeic stool
Stained stool smear examination
permanent stains such as iron-hematoxylin, or trichrome, are used to stain the stool sample before the microscopic observation of trophozoites
visible stained structures of Giardia intestinalis trophozoites include nuclei, adhesive discs, axostyles, and flagella
examination of a stool after concentration
formalin-ethyl acetate and zinc sulfate concentration methods are used to concentrate the stool so that the parasites have increased yield
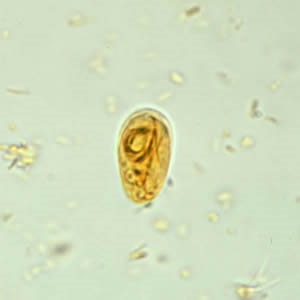
Image: G. lamblia cyst under a microscope (Source: CDC)
Stool Antigen (coproantigen) Detection:
based on the detection of a certain protein present on the wall of the parasite
monoclonal antibody-based capture Enzyme-Linked Immunosorbent assay (ELISA) and immunofluorescence assay (IFA) can be used to detect specific antigens in the stool
sensitivity of 88% - 98% and specificity of 87%- 100%
Culture
Stool cultures are not routinely performed for lab diagnosis of Giardia intestinalis.
Duodenal contents examination
it includes duodenal fluids and duodenal sampling
Duodenal fluid
in cases where giardiasis is suspected, direct examination of duodenal contents for trophozoites is done
the duodenal content such as mucus collected by entero-test or a string test
Entero-test
also known as string test
a gelatin capsule is tied to the end of a nylon string with a weight attached to it
the patient swallows the capsule while the other free end is taped to the cheek
the capsule is dissolved in the patient’s stomach, releasing the nylon string
since the string is attached to a weight, it travels down to the duodenum and jejunum
after 3-4 hours or overnight, while the patient maintains fasting, the string is pulled out
the bile stained mucus is then collected on a glass slide and immediately observed under a microscope of G. lamblia trophozoites
Duodenal sampling
done when repeated stool examination gave negative results but the parasitic infection is strongly suspected
by oesophagogastric-endoscopy, duodenal biopsy, or aspirates are obtained
the duodenal samples can also be retrieved by using a Cavey’s tube or Rubin’s tube
the samples are transferred to a glass slide by gently rubbing into it followed by standing by Giemsa and Trichrome stain
although this method has a high sensitivity, it is not frequently done as it is invasive and expensive
Serodiagnosis
IIF, ELISA can be used to detect serum antibodies specific to Giardia intestinalis
however, the tests cannot differentiate between recent and past infections so acute giardiasis can't be properly diagnosed
axenically cultured Giardia intestinalis trophozoites can be used as antigens in test assays
Molecular
DNA probes
PCR
Treatment of Giardia intestinalis
Durg of choice for giardiasis caused by Giardia intestinalis includes:
- Nitroimidazole derivates (metronidazole, tinidazole)
- acridine dyes (quinacrine)
- nitrofurans (furazolidone)
Prevention, Control of Giardia intestinalis
Prevention, Control of Giardia intestinalis are done by:
Individual prophylaxis
Individual prophylaxis of Giardia intestinalis is done by
improved personal hygiene such as proper washing of hands with soap after defecation and before eating food
treatment of water before drinking such as boiling, filtering the water used in a 0.22-micrometer membrane, iodination with tetracycline hydro per iodide
drinking bottled water while traveling to areas endemic to amoebiasis as chlorine treatment cannot kill the cysts
if salad is to be consumed, treat the vegetables with acetic acid or vinegar for 15 minutes
not performing sexual acts that involve fecal-oral contact
Community prophylaxis
Community prophylaxis of Giardia intestinalis is done by
improvement of the water management system to avoid fecal contamination
improvement of sanitation by installing latrines for proper disposal of human feces