Leishmania donovani - Pathogenesis, Pathology, Host Immunity
Pathogenesis of Leishmania donovani
Visceral leishmaniasis, caused by Leishmania donovani, is characterized by heavy parasitization of external organs and proliferation and destruction of reticuloendothelial cells of the internal organs.
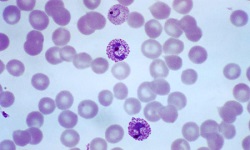
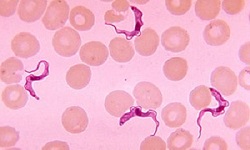
after a bite by a female sandfly infected with Leishmania donovani, the promastigotes are deposited on the surface of the host skin.
in addition, the sandfly also produces substances that deactivate the fixed macrophages in the skin which promotes the infectivity of the parasite.
through an alternative pathway, the host complement system is activated resulting in the production of C3b or C3bi
two specific receptors are present on the outer membrane of the promastigotes- a 63 kDa molecular weight glycoprotein and a lipophosphoglycan (LPG) – bind directly with the host macrophage’s CR3 and CR1 or indirectly through bound C3b or C3bi
the promastigotes phagocysed by macrophages transform into amastigotes
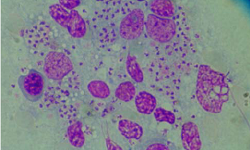
the newly formed Leishmania donovani amastigotes undergo binary fission inside the infected macrophages and after reaching a certain number (around 200), these enlarged macrophages bursts to release the amastigotes
the parasites then invade lymph nodes and reticuloendothelial systems of the spleen, liver, bone marrow
progressive hypertrophy occurs after macrophages present in the liver and spleen increases
in the spleen and the hematopoietic tissues of the bone marrow, lymphoid follicles are replaced by macrophages infected with amastigotes
the infected macrophages eventually replace normal hepatocytes in the liver
Pathology of Leishmania donovani
In leishmaniasis, the parasitized macrophages of reticuloendothelial systems are present in all parts of the body, but the majority of pathological changes are found in organs such as the spleen, liver, and bone marrow.
Spleen
spleen is grossly enlarged, soft, and fragile with the thickness of the capsule
the splenic pulp which is greatly increased and congested may turn purple or brown-black in Malpighian corpuscles
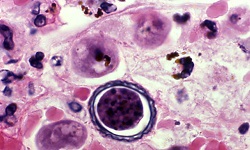
cells are densely packed with the amastigote form of Leishmania donovani
Liver
sharp edge, soft consistency, smooth surface, enlarged
Kupffer cells of liver are increased in size and number and are filled with the amastigote form of Leishmania donovani
in liver cells - fatty degeneration, swelling, and atrophic areas are seen
however, parasites are not found inside the hepatocytes
Bone Marrow
dark red in color
the extensive proliferation of reticuloendothelial cells including plasma cells can be observed
a large number of parasitized macrophages replace the hematopoietic tissues of the bone marrow
Lymph Nodes
enlarged lymph nodes
amastigotes demonstrated in China and the Mediterranean visceral leishmaniasis but not in the Indian kala-zar
Other Organs
other organs such as kidneys of infected individuals show cloudy swelling and the presence of macrophages infected with amastigotes
although the parasites are absent from the myocardium, the heart is pale in color
Host Immunity of Leishmania donovani
Leishmaniasis, also known as the disease of the immune system, is an immunologically bipolar disease – localized cutaneous disease from one pole and visceral or diffuse cutaneous disease on the other pole
localized cutaneous disease caused by Leishmania donovani induces a strong immune response and in most cases is resolved without intervention
the resolution of the disease is mediated by helper T-cell subtype 1 (TH1) immune response, Interferon g, Interleukin 2, and interleukin 12
the visceral or diffuse cutaneous disease involves unresponsiveness (anergy) to Leishmania donovani antigens and the infection is mediated by helper T-cell subtype 2 (TH2) cytokine immune responses
malnourished and young individuals are much more susceptible to leishmaniasis
Host immunity in visceral or diffuse cutaneous leishmaniasis, caused by Leishmania donovani, involves:
Specific inhibitions of cell-mediated immunity
Profound hyperglobulinaemia
Specific inhibitions of cell-mediated immunity
during visceral or diffuse cutaneous leishmaniasis, delayed hypersensitivity reaction, which can be detected by leishmania skin test is absent
the absence of delayed hypersensitivity reaction is also seen in in-vitro lymphocyte responses to leishmanial antigen
protection from Leishmania donovani infection occurs through the intact cell-mediated immunity
Profound hyperglobulinaemia
profound hyperglobulinaemia is caused by polyclonal lymphocyte activation
the host complement system is activated and immune complexes are formed
characterized by the large volume of production of specific anti-leishmanial antibodies and polyclonal non-specific immunoglobulins such as IgG
circulating antibodies do not protect the host from his infection
even during re-infection by Leishmania donovani, the individuals are not protected from kala-azar
the release of cytokines such as tumor necrosis factor and interleukins may aid in anorexia and wasting away