Paragonimus westermani - Host Immunity, Clinical Manifestation, Complication, Prognosis
Host Immunity of Paragonimus westermani
In parasitic infection by Paragonimus westermani, the host immune response includes an elevated level of specific antibodies in the host serum. However, these circulating antibodies do not give any protection against the infection.
Cell-mediated immunity (CMI) is also induced. It is responsible for delayed hypersensitivity which may persist for several years even after the infection has been cured.
Clinical Manifestations of Paragonimus westermani
The incubation period is between 10 to 12 weeks. In light infections, paragonimiasis is asymptomatic i.e. clinical manifestations of Paragonimus westermani are absent.
Acute paragonimiasis
Symptoms in acute paragonimiasis, which lasts for several weeks, include diarrhea, urticaria, and abdominal pain which is related to the invasion of the intestine and migration of larvae. These clinical manifestations of Paragonimus westermani are followed by fever, cough, chest pain, night sweat, dyspnoea, etc.
Chronic paragonimiasis
In chronic clinical manifestations of Paragonimus westermani, the disease may manifest as pulmonary paragonimiasis or extra-pulmonary paragonimiasis depending upon the area in which the parasite is residing.
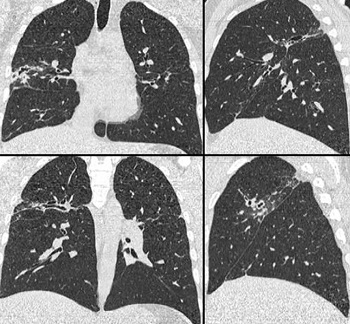
Image: Paragonimus westermani causing Pulmonary paragonimiasis (Source: archbronconeumol.org)
Pulmonary paragonimiasis
a most common form of infections
common symptoms include night seat, pleurisy pain, cough, rusty or golden brown sputum, recurrent bacterial pneumonia (secondary infection)
other clinical syndromes, which usually occur 6 months after infection, include eosinophilia, hemoptysis which is aggravated by exercise or intense physical work
as the disease progresses, other syndromes are observed
* presence of lung abscess or pleural effusion
* exudative effusion which contains eosinophils, Charcot-Leyden crystals
* lesions progress to form cystic fibrosis and eventual calcification in the lungs
since it mimics pulmonary tuberculosis, confusion or misdiagnosis may occur
Extra-pulmonary paragonimiasis
Extra-pulmonary paragonimiasis is much more severe and occurs due to the migration of Paragonimus westermani larvae or the introduction of eggs into body circulation.
It is of following types:
Abdominal paragonimiasis
Cerebral paragonimiasis
Subcutaneous paragonimiasis
Miscellaneous paragonimiasis
Abdominal paragonimiasis
Symptoms of abdominal paragonimiasis include abdominal mass, abdominal pain, muco-sanguineous diarrhea

Image: Paragonimus westermani causing abdominal paragonimiasis (Source: ReseachGate)
Cerebral paragonimiasis
cerebral paragonimiasis clinically resembles cerebral cysticercosis
clinical manifestations include convulsions, jacksonian epilepsy, cephalgia, hemiplegia, paresis, and visual disorders such as optic atrophy, papilloedema
is rare - occurs in less than 1% of symptomatic cases
Subcutaneous paragonimiasis
subcutaneous paragonimiasis includes the presence of swelling or subcutaneous nodules- found in the inguinal region as well as the lower abdomen
these nodules are tender, firm, and mobile which can contain developing Paragonimus westermani
Miscellaneous paragonimiasis
miscellaneous paragonimiasis of extra-pulmonary paragonimiasis includes various sites where Paragonimus westermani may be present
includes liver, spleen, kidney, testes, ovary, mesenteric lymph nodes
Complications of Paragonimus westermani
Complications of Paragonimus westermani in pulmonary paragonimiasis are lung abscess, pleural effusion, and empyema.
Complications of Paragonimus westermani in cerebral paragonimiasis are seizures and coma.
Prognosis of Paragonimus westermani
If acute paragonimiasis is left untreated, death may occur.
For pulmonary paragonimiasis, specific treatment is required. Within a few weeks of treatment, eggs from sputum and clinical syndromes associated with the condition are resolved.
In cerebral paragonimiasis, the prognosis is poor with a mortality rate of 5% in untreated cases.
The prognosis of Paragonimus westermani for miscellaneous paragonimiasis is also bad.