Paragonimus westermani - Laboratory Diagnosis, Treatment, Prevention, Control
Laboratory diagnosis of Paragonimus westermani
The laboratory diagnosis of Paragonimus westermani includes:
Specimen
Sputum
Feces
* eggs are detected in samples 2 to 3 months after infection.
Microscopy
Diagnosis of pulmonary paragonimiasis is based on a demonstration of operculated Paragonimus westermani eggs in the sputum of feces.
Sputum Microscopy
sputum (not saliva) should be collected in the morning and immediately examined
if sputum is highly muscoid or viscous, it is treated with an equal volume of 3% sodium hydroxide (NaOH)
saline or iodine wet-mount microscopy is usually done – first under low power and then under high power
the concentration of sputum can be done by the formalin-ether sedimentation method
demonstration of golden-brown operculated eggs confirms pulmonary infection by Paragonimus westermani
since sensitivity is 25% to 30%, repeated samples should be examined – upto 7 samples must be collected at different intervals during 15 day period
Stool Microscopy
usually important in children as they have the habitat of swallowing the sputum
at least 3 stool samples must be examined for Paragonimus westermani eggs during 7 days period

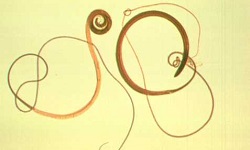
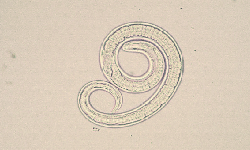
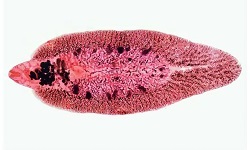
Image: Paragonimus westermani adult (Source: CDC)
Immunodiagnosis
Detection of antibodies
Since Paragonimus westermani induces immune response i.e. presence of circulating antibodies, serological methods can be used for laboratory diagnosis. Crude extract of adult Paragonimus westermani retrieved from laboratory cats is used as antigen in these assays.
Serological tests used to detect serum antibodies include
Complement fixation test
* has prognostic value as this test does not detect antibodies after specific therapy
Indirect haemagglutination
Counter-current immunoelectrophoresis
Latex agglutination
Western Blot (sensitivity- 96%, specificity- 99%)
These tests may show false positive/ cross-reactivity with Fasciola hepatica but do not detect antibodies to other Paragonimus species.
Disadvantages of serological tests
A major disadvantage of serological methods is that antibody levels against Paragonimus westermani remain high even up to 2 or more years after successful treatment.
Advantages of serological tests
The advantages of Serodiagnostic methods:
diagnosis during the pre-patent period during which eggs have not yet been released in stool or sputum
in cases of extra-pulmonary paragonimiasis as eggs are not found in the stool or sputum
Skin Test
The intradermal skin test for Paragonimus westermani infection is a simple and reliable test:
Procedure
saline extract of the parasite i.e. antigen diluted at 1:2000 is intradermally injected (0.1ml) in one arm
an equal volume of normal saline is injected intradermally on the other arm as a control
development of a large wheel, pseudopodium, or erythema after 15 minutes to 30 minutes indicates infection
Even after successful treatment, this test may be positive from 1 year to 20 years. Thus, it is used for epidemiological studies rather than diagnostic methods.
Imaging Methods
The imaging methods are most useful to differentiate between paragonimiasis and tuberculosis. Some tests used for Paragonimus westermani diagnosis include:
X-ray: for pulmonary paragonimiasis
CT- scan: for cerebral paragonimiasis
MRI: for cerebral paragonimiasis
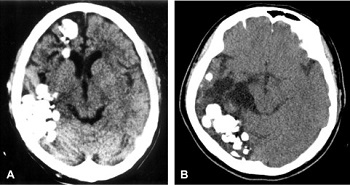
Image: Paragonimus westermani causing cerebral paragonimiasis (Source: ScienceDirect)
Treatment of Paragonimus westermani
Drugs of choice for the treatment of Paragonimus westermani infection are Praziquantel, Bithionol, and Niclofolan.
Prevention, Control of Paragonimus westermani
The control and prevention of Paragonimus westermani can be obtained by following steps:
avoid consumption of raw/undercooked meat, crayfish, crabs
proper filtration and/or boiling of drinking water
immediate treatment of infections in pigs, cattle, and people
use of molluscicides to control snails
reduce contamination of water sources by infected animals, and human feces as well as sputum