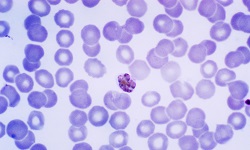
Plasmodium falciparum - Host Immunity
Host Immunity of Plasmodium falciparum
Two types of host immunity are developed against Plasmodium falciparum malaria:
Natural/innate immunity
Acquired immunity
Natural/innate immunity
Natural or innate immunity includes inherent but non-immune mechanisms against Plasmodium falciparum malaria. This host defense depends on the nature of the red blood cells such as:
Age of Red Blood cells
nature of hemoglobin
enzyme content of erythrocytes
Age of Red Blood cells
In contrast to P. vivax and P. ovale which infect only young erythrocytes, Plasmodium falciparum infects both young as well as old erythrocytes.
Nature of hemoglobin
Some genetic disorders which result in the formation of abnormal hemoglobin molecules result in resistance to malaria disease. These factors include:
Haemoglobin S (HbS) - sickle cell anemia trait
Thalassemia hemoglobin
Fetal hemoglobin
Haemoglobin S (HbS) - sickle cell anemia trait
genetically inherited trait responsible for natural resistance against Plasmodium falciparum
this condition involves Haemoglobin S (HbS) when exposed to low oxygen tension fails to host the growth of malarial parasite- probably due to potassium escaping from such parasitized cells
as a result, the parasitized RBC becomes rigid, sickle-shaped, and are phagocytosed
the phagocytosed parasites are immediately developed before they are able to develop into schizonts
this trait is commonly seen in some areas of Asia, Africa, and Europe
Thalassaemia hemoglobin trait
This hereditary trait provides protection against Plasmodium species
Fetal hemoglobin
This hereditary trait provides protection against Plasmodium species including Plasmodium falciparum
Enzyme content of erythrocytes
Another genetic trait is the Glucose-6-phosphate dehydrogenase (G6PD) deficiency trait. Although the exact protective mechanism is not understood, it is believed to have occurred by interfering with the adaptability of the parasite to the G6PD deficient condition of the RBCs.
Acquired immunity
The acquired immunity restricts the level of parasitemia and eventually provides protection from the disease but not the infection. The development of immunity is a result of a complex interaction between Plasmodium falciparum and the host immune system- both humoral immunity and cell-mediated immunity.
Humoral immunity
in individuals repeatedly exposed to Plasmodium, the development of circulating antibodies against sporozoites, asexual blood stages, and sexual blood stages of the parasite is developed
while the asexual stages of the parasite have consequently evolved various methods for immune evasion, the antibody response is strongest against the parasites in these development stages
the humoral immunity against asexual stages provides protection by
* inhibiting RBC invasion
* inhibiting growth inside the RBC
* sequestration of parasitized RBC
the humoral antibodies provide protection by decreasing the susceptibility of the host to malarial infection as well as disease
antibodies against sexual stages help in reducing malaria transmission
Acquired antibody-mediated immunity is transferred from mother to fetus through the placenta which protects the infant from severe malaria in the first few months after birth – usually for 6 months to 9 months
Cell-mediated immunity
cell-mediated immunity provides the non-specific type of immunity through numerous cellular mechanisms against Plasmodium falciparum
in acute cases, a correlation has been found between natural killer (NK) activity and resistance to malaria
activated macrophages phagocytose and induce extra-cellular killing of target cells which may be specifically amplified or induced by antibodies bound to target cell surfaces
this non-specific process may also be activated by endotoxin-like substances derived from malaria parasites
activated macrophages also release mediators which are responsible for various pathological changes
naturally acquired immunity is immunocompromised individuals including pregnant women- especially primigravida