Plasmodium falciparum - Prognosis, Epidemiology, Reservoir, Transmission, Treatment, Prevention, Control
Prognosis of Plasmodium falciparum
In uncomplicated cases of Plasmodium falciparum malaria, when detected at an early stage, the prognosis is good. With the administration of antimalarial drugs, improvement is seen within 48 hours and the patient is free of fever after 96 hours.
If not treated quickly and completely, the prognosis of PPlasmodium falciparum infection is not good with a high mortality rate. Children under five and non-immune populations also have a bad prognosis.
Cerebral malaria has a high mortality rate- at 25% even if treated with anti-malarial drugs. Survivors may suffer from sequelae including aphasia, hemiparesis, spasticity, and cerebellar ataxia.
Epidemiology of Plasmodium falciparum
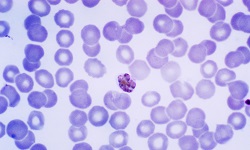
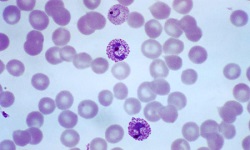
Plasmodium falciparum is the most dangerous and life-threatening malaria species to humans. The disease is widely prevalent in tropical areas below the altitude of 1000m.
The malaria infection is endemic to Africa, Haiti, New Guinea, Oceania, South America, South-East Asia, and Central America. Plasmodium falciparum also occurs in Sri Lanka, Pakistan, Bangladesh.
Reservoir, Source of Plasmodium falciparum
Man is the only source of Plasmodium falciparum. Individuals suffering from acute malaria and chronic malaria harboring gametocytes are reservoirs of the malaria parasite.
Natural vectors include female hematophagous Anopheles culicifacies and A. fluviatilis.
Transmission of Plasmodium falciparum
Plasmodium falciparum malaria is transmitted by:
bite of infected female anopheles mosquito during blood meal – the sporozoites are transmitted
blood transfusion from patients suffering from parasitemia but lacking typical malaria symptoms such as fever – the merozoites are transmitted
transplacental transmission – congenital malaria
organ transplantation
Treatment of Plasmodium falciparum
Treatment of Plasmodium falciparum infection is based on
specific antimalarial chemotherapy
suppurative therapy
Specific antimalarial chemotherapy
Although such a drug is not yet available, antimalarial drugs are designed to destroy:
- all asexual forms of parasites in the blood
- hypnozoites to prevent relapse and extra-erythrocytic forms
- gametocytes to cease transmission of infection
Antimalarial drugs function by inhibiting the growth of malarial parasites by increasing the internal pH of parasites by concentration within acid vesicles of a parasite as well as inhibiting the utilization of hemoglobin and metabolism of the parasite.
some antimalarial drugs are:
- common: chloroquine, amodiaquine, chloroguanide, pyrimethamine, quinacrine hydrochloride, primaquine, proguamil, quinine
- newer drugs are used to treat chloroquine-resistant Plasmodium: artemisinin and its derivatives, mefloquine, sulfonamides such as sulfadoxine
Supportive therapy
supportive therapy and treatment of complications of Plasmodium falciparum malaria are important aspects of the management of malaria infection. These supportive treatments include:
cooling blankets and antipyretics to treat hyperthermia
electrolyte and fluid balance to maintain cardiac output, renal perfusion, and to prevent fluid overload
anticonvulsants to treat seizures in cases of cerebral malaria
for pulmonary edema, incubation and assisted ventilation takes place
in cases of hypoglycemia, parenteral glucose infusion is required
blood transfusion to treat severe anemia
exchange blood transfusion to treat hyperparasitemia in cases of
more than 15% of parasitemia
more than 5% parasitemia and cerebral malaria
evidence of organ dysfunction
Prevention, Control of Plasmodium falciparum
The prevention and control of Plasmodium falciparum infection are based on
successful treatment of infected individuals
reduction of transmission by controlling mosquito population especially around housing by eliminating breeding places, spraying oils and chemicals in breeding sites
using mosquito nets while sleeping, and netted windows in endemic areas
wearing protective clothing
use of mosquito repellants
chemoprophylaxis
Vaccine of Plasmodium falciparum
Vaccines are not available despite intensive research since the mid-1970s.