Cystoisospora belli - Life Cycle, Pathogenesis, Pathology, Host Immunity, Clinical Manifestation
Life Cycle of Cystoisospora belli
The transmission of Cystoisospora belli takes place by the faecal-oral route.
Susceptible human hosts, usually with compromised immune systems, acquire infection by drinking water or consuming food contaminated with mature Cystoisospora belli oocysts
upon reaching the small intestine, these mature oocysts excysts to release the sporozoites
the sporozoites invade the enterocytes of the proximal jejunum and distal duodenum
inside the enterocytes, they undergo asexual multiplication (schizogony)
the schizogony cycle releases merozoites after rupturing the schizonts
the merozoites invade new host epithelial cells
Cystoisospora belli trophozoites eventually develop into schizonts which contain many merozoites
trophozoites undergo sporogony (sexual cycle) after a week to produce macrogamont (female) or microgametocyte forms (male)
each microgametocytes produce microgametes which are spermlike and fertilize the macrogamont
as a result of fertilization, unsporulated oocysts are formed
each unsporulated oocyst contains a single sporoblast and is excreted in the faeces
the oocysts mature outside the body in the environmental conditions
after sporulating, mature oocysts contain two sporocysts, each containing four sporozoites
these mature oocysts are infectious to humans and can remain resistant and viable in the environment for months
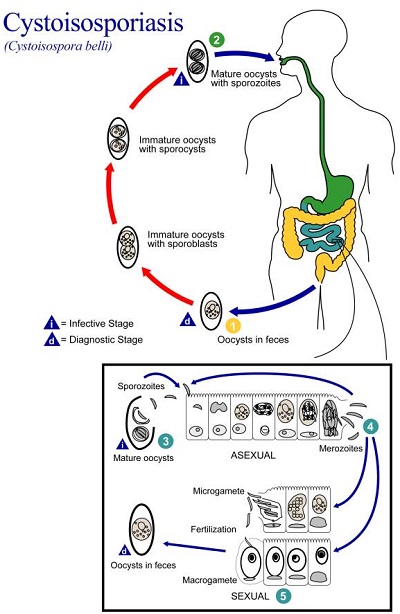
Figure: Cystoisospora belli life cycle (Source: CDC)
Pathogenesis, Pathology of Cystoisospora belli
Pathogenesis of cystoisosporiasis includes invasion and subsequent damage of the epithelial cells of the proximal jejunum and distal duodenum. The host cells are believed to have been damaged through a toxin-mediated mechanism, although no toxin has been identified.
Non-specific changes include shortened villi, mucosal atrophy, hypertrophic crypts, and lamina propria infiltrated with eosinophils and other inflammatory cells.
Cystoisospora belli infection is limited to the gastrointestinal tract in most cases. Cases involving extraintestinal forms of the disease have been reported in AIDS patients.
Host Immunity of Cystoisospora belli
The host immune response responsible for clearing the Cystoisospora belli parasite from the gut is under study and not understood.
Clinical Manifestation of Cystoisospora belli
the incubation period is 3-14 days
the main clinical syndrome/manifestation of Cystoisospora belli includes diarrhoea without blood and inflammatory cells
diarrhoea is watery, profuse, and foul smelling
other symptoms include abdominal pain, weight loss, occasional malabsorption, peripheral eosinophilia
in immunocompetent hosts, Cystoisospora belli causes self-limiting mild diarrhoea
in patients with AIDS, it causes chronic, life-threatening diarrhoea as well as dehydration
Complications of Cystoisospora belli
In immunocompromised hosts and young hosts, the most common complication of Cystoisospora belli infection is severe dehydration.
Cases involving extra-intestinal forms and subsequent disease complications have been reported in AIDS patients. Haemorrhagic colitis has also been reported in cystoisosporiasis.
Prognosis of Cystoisospora belli
Cystoisospora belli infection is self-limiting in otherwise healthy hosts.
The prognosis is excellent with therapy.
The parasitic infection presents as chronic, life-threatening diarrhoea as well as dehydration in AIDS patients.