Cystoisospora belli - Laboratory Diagnosis, Treatment, Prevention, Control
Laboratory Diagnosis of Cystoisospora belli
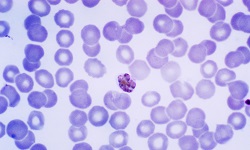
Since cystoisosporiasis clinically resembles giardiasis, cryptosporidiosis, and cyclosporiasis, the clinical diagnosis is difficult. Identification and demonstration of Cystoisospora belli oocysts in the specimen are made for the diagnosis of infection.
Sample
stool
duodenal or jejunal aspirations
Microscopy
Microscopic examination of the specimen after wet mount preparation and stained smear preparation is done to determine the presence/absence of oocysts. Stains such as Rhodamine, haematoxylin and eosin, Giemsa stains can be used.
Since Cystoisospora belli oocysts are excreted variably in the stool, multiple stool samples should be examined. Also, the concentration of stool by methods such as formalin-ethyl acetate sedimentation and Sheather’s sucrose concentration can be used to concentrate the oocysts before microscopic examination.
Direct Wet mount examination
Epifluorescence
Acid-fast staining of stool smear
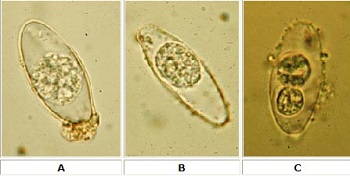
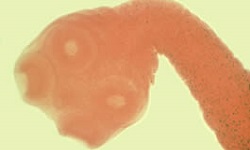
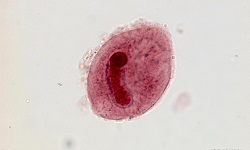
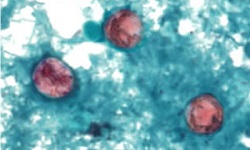
Image: Cystoisospora belli cysts; A, B - immature oocyst; C - maturing cyst with two sporoblasts (Source: wikidoc.org)
Direct Wet mount examination
Direct wet mount examination is useful with stool specimens with a high to moderate number of oocysts
presence of elliptical-shaped Cystoisospora belli oocysts confirms the parasitic infection
direct stool wet mount method using bright-field microscopy and differential interference contrast (DIC) microscopy can be done
Lacto Phenol Cotton Blue wet mount also be used to demonstrate deep blue stained oocysts
Epifluorescence
under ultraviolet rays, oocysts have the property of demonstrating autofluorescence
use of 450-490 excitation filter reveals the presence of fluorescent oocysts under epifluorescence illumination
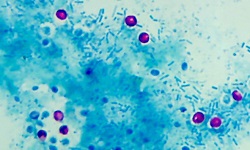
Acid-fast staining of stool smear
Cystoisospora belli oocysts are acid-fast
pink coloured acid-fast oocysts can be seen in samples after staining by the Ziehl-Neelsen method
Entero-test
Entero-test is also known as string test
also done for diagnosis of Cystoisospora belli infection
a gelatin capsule is tied to the end of a nylon string with a weight attached to it
the patient swallows the capsule while the other free end is taped to the cheek
the capsule is dissolved in the patient’s stomach, releasing the nylon string
since the string is attached to a weight, it travels down to the duodenum and jejunum
after 3-4 hours or overnight, while the patient maintains fasting, the string is pulled out
the bile stained mucus is then collected on a glass slide and immediately observed under a microscope
Endoscopy
Done if repeated stool specimen examination gives a negative diagnosis for Cystoisospora belli but strong suspicion of Cystoisospora belli remains. Upper gastrointestinal endoscopy is collected for demonstration of oocysts in the biopsy specimen.
Serodiagnosis
There are no serological tests for laboratory diagnosis of Cystoisospora belli.
Treatment of Cystoisospora belli
Drugs used for the treatment of Cystoisospora belli is oral co-trimoxazole (trimethoprim, sulfamethoxazole)
Prevention, Control of Cystoisospora belli
Prevention, Control of Cystoisospora belli are done by:
Individual prophylaxis
Individual prophylaxis of Cystoisospora belli is done by
improved personal hygiene such as proper washing of hands with soap after defecation and before eating food
treatment of water before drinking such as boiling, filtering the water used in a 0.22-micrometre membrane, iodination with tetracycline hydro per iodide
drinking bottled water while travelling to areas endemic to cyclosporiasis as chlorine treatment cannot kill the cysts
if salad is to be consumed, treat the vegetables with acetic acid or vinegar for 15 minutes
not performing sexual acts that involve faecal-oral contact
Community prophylaxis
Community prophylaxis of Cystoisospora belli is done by
improvement of the water management system to avoid faecal contamination
improvement of sanitation by installing latrines for proper disposal of human faeces