Schistosoma japonicum - Clinical Manifestation, Complication, Epidemiology, Reservoir, Transmission
Clinical manifestations of Schistosoma japonicum
Schistosoma japonicum can cause acute schistosomiasis or chronic schistosomiasis in the intestines and liver and rarely in the lungs and host central nervous system. However, it is more severe and profound than in other Schistosoma infections.
Acute schistosomiasis
Cercarial dermatitis
also called swimmer’s itch
cercarial dermatitis is rarely a primary infection and mostly occurs in previously exposed individuals
infection may be acquired from both freshwater and saltwater
within 24 hours of infection, a pruritic rash occurs
Katayama fever
commonly in infections caused by Schistosoma mansoni and Schistosoma japnicum infections
the incubation period for Katayama fever is 4 weeks to 6 weeks
serum-like sickness occurring at the time when the first egg batch is released in the intestine
common symptoms include fever, chills, weakness, diarrhoea, myalgia, and right upper quadrant pain while rare symptoms are non-productive cough, rash, anorexia, headache, and eosinophilia (40% cases)
although the symptoms resolve after several weeks, the condition may become fatal if left untreated
Chronic schistosomiasis
Schistosoma japonicum infections are mostly asymptomatic or mildly symptomatic while clinical syndromes are present in heavy infections. The onset of chronic schistosomiasis is insidious.
Intestinal schisosomiasis
intestinal schistosomiasis is caused by the formation of granuloma along the intestinal wall and retention of Schistosoma japonicum eggs
clinical symptoms include schistosomiasis dysentery (mucosal diarrhoea), abdominal pain, bloody stool along with the passage of parasite eggs
in cases of heavy infections, recurrent Salmonella infection with negative stool culture but with positive blood cultures is seen
occurs in the small intestine
Hepato-splenic schisosomiasis
hepato-splenic schistosomiasis occurs when the Schistosoma japonicum infection spreads to the liver
associated with portal hypertension, ascites, periportal fibrosis, and splenomegaly
during the early stages, common symptoms include pain in the left hypochondrium, dyspepsia, flatulence
in later stages symptoms includes melena, haematemesis, oedema of the lower, abdominal distension
if toxic hepatitis and other infections in the liver occurs, liver failure may occur
Cerebral schisosomiasis
more common (2% to 4% of cases) in Schistosoma japonicum infection than in Schistosoma mansoni
symptoms include headache, myeloradiculopathy, seizures, paresthesia, bladder dysfunction, etc
Complications of Schistosoma japonicum
Complications of Schistosoma japonicum which are more rapid than other Schistosoma infections includes Symmers clay pipe stem fibrosis or liver fibrosis, cor-pulmonale, intestinal fibrosis, and pulmonary hypotension.
Epidemiology of Schistosoma japonicum
Schistosoma japonicum infections are restricted to four countries of Western Pacific and South-East Asia – China, Philippines, Indonesia, and Thailand.
Reservoir, Source of Schistosoma japonicum
The definitive hosts - man, domestic animals (cat, dog, cattle, pig), and wild animals (mouse, monkey, feline, mustelid) – are important reservoirs, and sources for Schistosoma japonicum. Since the parasite eggs are excreted in the animal faeces more than in man, they are a more important reservoir than a man.
The intermediate host - amphibian snails of the genus Oncomelania – are important in maintaining parasitic infections.
Transmission of Schistosoma japonicum
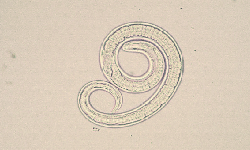
Schistosoma japonicum is transmitted from one person to another after coming in close physical contact with water infested with the cercariae of the parasite. The cercariae penetrate the skin of the man to cause infection.