Trypanosoma cruzi - Life Cycle, Pathology, Pathogenesis, Host Immunity
Life Cycle of Trypanosoma cruzi
The life cycle of Trypanosoma cruzi completes in two hosts
Mammals (including man)
Reduviid bugs
* Other vertebrates such as amphibians, birds, and reptiles are resistant to infection from Trypanosoma cruzi.
transmission of Trypanosoma cruzi infection begins when the reduviid bugs feces containing metacyclic trypomastigotes come in direct contact with the mucous membrane, conjunctiva, or broken skin of the mammal host
also, when the reduviid bugs bite and feed on the blood of the mammals, the feces are deposited on the surface of the skin
after the parasites are introduced into the host, they transform into intracellular amastigotes at the site of entry
inside the host cell, the amastigotes of Trypanosoma cruzi multiply
once the infested host cell is completely filled with amastigotes, they differentiate into trypomastigotes
after the differentiation into trypomastigotes are complete, the host cells rupture
these newly released Trypanosoma cruzi trypomastigotes enter the circulatory system of the host but do not multiply
the lymphatic system and blood of the host carry these trypomastigotes to distant body parts such as the skeletal muscles, cardiac muscles, nervous system cells, and intestinal muscles of the gastrointestinal tract
In these tissues, the Trypanosoma cruzi trypomastigotes transform into amastigotes
these amastigotes undergo binary fission to form pseudocysts, a mass of parasites
in a short time of five days, in each pseudocyst, one trypomastigote may divide to form nearly 500 amastigotes
the amastigotes present in the pesudocyst transform into epimastigotes and eventually into trypomastigotes
these trypomastigotes are released back into the circulatory system of the host
during a blood meal from an infected man by reduviid bugs, the Trypanosoma cruzi trypomastigotes are picked up
when the trypomastigotes reach the midgut and gut of the vector, they are transformed into amastigotes and gradually into epimastigotes
the epimastigotes multiply to give a large number of the parasite
when these epimastigotes reach the rectum of the insect vector, they change into non-diving metacyclic trypomastigotes
within 8-10 days, these metacyclic trypomastigotes are passed out into the feces of the bug and the life cycle continues
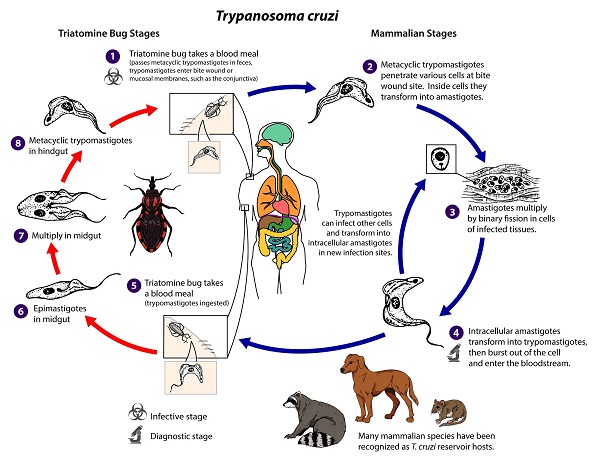
Figure: Trypanosoma cruzi LifeCycle (Source: CDC)
Pathogenesis of Trypanosoma cruzi
The pathogenesis of acute Chagas’ disease, caused by Trypanosoma cruzi, depends on the destruction of first infected host cells and then non-parasitized host cells. The destruction of the host cells is responsible for the clinical symptoms of the disease
Pathology of Trypanosoma cruzi
The pathology of Trypanosoma cruzi includes:
Acute Chagas’ disease
Acute Chagas’ disease is characterized by a typical lesion that first appears at the site of Trypanosoma cruzi metacyclic trypomastigotes entry
involves the localized swelling of the skin
the presence of intracellular amastigotes in the host leucocytes as well as subcutaneous tissues
in cases of dissimilated cases, pseudocysts are present
the inflammatory response is intense
parasitemia may occur
Chronic Chagas’ disease
in chronic cases called Chronic Chagas’ disease, Trypanosoma cruzi infection pathological lesions by inducing an inflammatory response, cellular lesions, and fibrosis
the inflammatory response is caused by the release of trypomastigotes after the rupture of infected host cells, cellular debris as well as inflammatory parasitic molecules
the inflammatory response is less intense as the infection has been partially controlled by the host's immune response
these lesions occur mostly in the esophagus, colon, and heart- although any host organ such as gall bladder and urinary bladder may be involved
cytolysis of myocytes and autonomic denervation of the nerve cells are associated with cellular lesions
the lesions are caused by the direct destruction of cells by parasitic multiplication, necrosis as a result of inflammation, and cytotoxic activities of the CD8 T cells and CD4 T cells
after lesions eventually heals by fibrosis and regression occurs by difficulty
in cases, of Chagas’ disease associated with myocardiopathy, cardiac dilation, and failure may occur as a result of extensively destroyed myocytes replaced by fibrosis, hypertrophy of remaining myocytes
although the Trypanosoma cruzi parasites are rarely demonstrated in the myocytes, the thinning of the left ventricle wall which results in the formation of an apical aneurysm may occur
conditions such as Megaoesphagus, and megacolon arise after the esophagus, stomach, and colon of the host become enormously dilated, enlarged, and hypertrophied
the mega disease of other organs such as the gall bladder and urinary bladder may also take place
Host Immunity of Trypanosoma cruzi
the host immune response of Trypanosoma cruzi is rapid, vigorous
includes both humoral and cell-mediated immunity (CMI)
Humoral
the circulating antibodies are not protective in the initial stages and appear three or more weeks after infection
they destroy the Trypanosoma cruzi parasites by lysis – thus eliminating them from the host circulatory system
however, once the parasites become intracellular, antibodies provide no protection against the parasites
Cell-mediated immunity (CMI)
Cell-mediated immunity (CMI) is mediated through macrophages and is dependent on the lymphocyte
Cell-mediated immunity (CMI) is also responsible for killing intra-cellular amastigotes present inside the host tissues